Background
Traditional methods of breast reduction involve remodeling the breast mound based on an inferior, superior, or central pedicle and then trimming and redraping the skin over the new shape. Unfortunately, these techniques necessitate long scars. Minimizing scars in breast surgery has been an important goal in the previous 2 decades, with many techniques developed specifically for this purpose. [1]
Among them is round block mammaplasty, described by Benelli in 1990, which produces only a periareolar scar. [2] In 1987, Lassus modified a technique described in the mid 1960s, producing a periareolar and vertical scar. [3] In the late 1980s, Lejour applied suction lipectomy as an adjuvant to surgical resection in female macromastia. [4]
Liposuction is one of the most commonly performed procedures in plastic surgery and has been used safely in many body regions. Several authors have reported on the safety and efficacy of suction lipectomy, power-assisted liposuction, and ultrasound-assisted lipoplasty (UAL) in gynecomastia. [5, 6, 7, 8, 9, 10]
In 1991, Matarasso and Courtiss described their results using suction mammaplasty to reduce moderate breast hypertrophy in the absence of ptosis. [11] In 1993, Williams suggested liposuction of the breast to treat a unilateral hypertrophy in an adolescent breast maldevelopment. [12]
Skin retraction secondary to scarring in the superficial plane where traditional or superficial liposuction is performed is a well-known phenomenon; a controlled iatrogenic tightening of the skin envelope is produced.
In 1997, the authors reported their experience in extending the indications to liposuction of the female breast in selected patients, even in large breast hypertrophy (resection >800 g). [13] Others have reported on breast reduction in females by liposuction-assisted procedures.
In 2004, Rohrich and colleagues reported that liposuction-only breast reduction had become one of the current techniques for breast reduction, with satisfactory results for both surgeons and patients. [12]
A prospective study by Abboud and Dibo reported power-assisted liposuction mammaplasty to be a safe and reliable means of breast reduction in patients with massive breast ptosis. The procedure, performed on 150 women (300 breasts) in the study, included creation of a lateral pedicle to maintain nipple-areola complex sensitivity. Wound infection, wound dehiscence, and seroma occurred in 2%, 1%, and 3% of breasts, respectively, with partial areolar necrosis occurring in two patients (1.3%) and revision surgery being performed in nine patients (6%). [14, 15]
A study by Wong and Malata indicated that UAL is more effective than conventional liposuction in the treatment of gynecomastia. The study, which included 219 patients (384 breasts), found the rate of intraoperative conversion to open excision to be 25% for UAL, compared with 39% for conventional liposuction, while the rate of postoperative revision was 2% for UAL, compared with 19% for conventional liposuction. [16]
For information on other breast reduction techniques, see the Breast section of Medscape Reference's Plastic Surgery journal.
Problem
Female breast hypertrophy or macromastia is a condition of abnormal enlargement of the breast tissue in excess of the normal proportion.
This condition may be caused by gland hypertrophy, excessive fatty tissue, or a combination of both. It varies in severity from mild (< 300 g) to moderate (300-800 g) to severe (>800 g).
Macromastia can be unilateral or bilateral and can occur in combination with ptosis, a term used when the nipple has descended below the inframammary crease.
Etiology
Large breasts frequently develop during pubertal breast development but also occur after pregnancy, weight gain at any age, or menopause.
Macromastia typically is caused by fat hypertrophy rather than glandular hypertrophy. Many females are destined genetically to have large breasts, which often is aggravated by pregnancy or weight gain. Iatrogenic causes include asymmetry following a mastectomy or lumpectomy. Rarely, a young patient may experience virginal mammary hypertrophy resulting in massive breast hypertrophy and a high recurrence rate following a reduction procedure.
Presentation
The typical patient presents with back pain, neck pain, breast pain, embarrassment, difficulty with sports, and clothing limitations. Those with more ptotic breasts develop intertrigo. Poor posture is common, and grooving of the shoulder from the force of the bra strap may occur. The patient may be overweight.
Indications
Breast liposuction is indicated when a minor-to-moderate reduction is requested and no ptosis correction is required. Other indications include the following:
-
Selected women needing larger reduction who do not want the scar associated with an open reduction or loss of sensation in their breasts and are willing to accept some ptosis
-
As a secondary mammaplasty procedure rather than an open revision
-
For asymmetry up to 1 cup size
-
In young patients with virginal hypertrophy, a condition with a high recurrence rate, as a temporary procedure before the end of the growth phase
Relevant Anatomy
The female breast normally grows during puberty under the influence of estrogen and progesterone. It is formed by 15-20 lobules of glandular tissue, each drained by a lactiferous duct. Each duct has an opening on the nipple. These lobules constitute the mammary gland and are interspersed with fat lobules. See the image below.
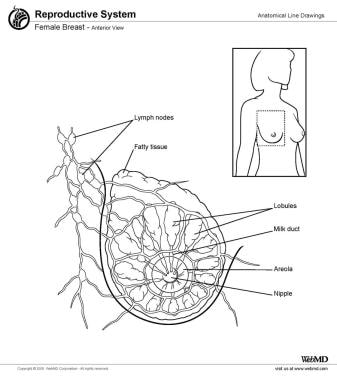
This fat tissue confers the rounded contour and most of the bulk of the breast (approaching 90%), except during pregnancy and lactation.
The abundant blood supply to the breast comes from perforators from the internal thoracic artery, external thoracic artery, thoracodorsal artery, and the third to fifth intercostal arteries.
Lateral and anterior cutaneous branches of the second to sixth intercostal nerves supply innervation of the breast. The third and fourth intercostal nerves most frequently innervate the nipple, but variations occur.
Any pattern of breast reduction involving parenchymal excision may disrupt nipple-areola sensation.
For more information about the relevant anatomy, see Breast Anatomy.
Contraindications
Mammography demonstrating breast hypertrophy to be mostly glandular contraindicates this procedure. Liposuction reduction mammaplasty is contraindicated in any female with mammographic findings that raise suspicion. Presence of ptosis and poor skin condition with little tissue elasticity also are contraindications to this procedure.
-
The skin is pierced 2 cm above the inframammary fold, in the mid line.
-
The right breast is infiltrated up to tumescence with solution; the left breast already has been infiltrated.
-
Appearance of the right breast after a liposuction of 700 mL.
-
Appearance of both breasts at the end of the procedure. The liposuction of the right breast is 700 mL; the liposuction of the left breast is 600 mL.
-
At the end of the procedure, elastic tape is used to mould the breast in the new shape and position.
-
Mammographic appearance of breast hypertrophy with a prevalence of fat tissue over glandular tissue. This mammographic image demonstrates the eligibility of the patient for liposuction of the breast to reduce the hypertrophy.
-
The material suctioned from the breast appears as a yellow, fatty, bloodless fluid.
-
A 22-year-old patient, preoperative view. Bra size is 40E. The distance from the jugular notch to the nipple is 33.5 cm on the right breast and 32 cm on the left breast.
-
Appearance 6 weeks after breast reduction by suction alone; 22-year-old patient. Preoperatively, bra size was 40E. The distance from the jugular notch to the nipple was 33.5 cm on the right breast and 32 cm on the left breast. During the procedure, 800 mL was removed from each breast. Postoperative bra size is 38C. The distance from the jugular notch to the nipple is 29 cm on the right breast and 28 cm on the left breast.
-
A 22-year-old patient, preoperative view. Bra size is 40E. The distance from the jugular notch to the nipple is 33.5 cm on the right breast and 32 cm on the left breast.
-
Appearance 6 weeks after breast reduction by suction alone; 22-year-old patient. Preoperatively, bra size was 40E. The distance from the jugular notch to the nipple was 33.5 cm on the right breast and 32 cm on the left breast. During the procedure, 800 mL was removed from each breast. Postoperative bra size is 38C. The distance from the jugular notch to the nipple is 29 cm on the right breast and 28 cm on the left breast.
-
Right lateral preoperative view; 22-year-old patient. Bra size is 40E. The distance from the jugular notch to the nipple is 33.5 cm on the right breast and 32 cm on the left breast.
-
Right lateral view 6 weeks after breast reduction by suction alone; 22-year-old patient. Preoperatively, bra size was 40E. The distance from the jugular notch to the nipple was 33.5 cm on the right breast and 32 cm on the left breast. During the procedure, 800 mL was removed from each breast. Postoperative bra size is 38C. The distance from the jugular notch to the nipple is 29 cm on the right breast and 28 cm on the left breast.
-
A 24-year-old patient, preoperative view. Preoperative bra size is 36DD. The distance from the jugular notch to the nipple is 25.5 cm on the right breast and 24.5 cm on the left breast.
-
A 24-year-old patient, view 6 weeks postoperatively. Preoperative bra size was 36DD. The distance from the jugular notch to the nipple was 25.5 cm on the right breast and 24.5 cm on the left breast. Postoperative bra size is 36C. The distance from the jugular notch to the nipple is 22 cm on each breast.
-
A 24-year-old patient, postoperative lateral view at dressing change. Preoperative bra size was 36DD. The distance from the jugular notch to the nipple was 25.5 cm on the right breast and 24.5 cm on the left breast. Postoperative bra size is 36C. The distance from the jugular notch to the nipple is 22 cm on each breast. Note the ecchymosis on the lateral part of the breast.
-
A 24-year-old patient, postoperative view at first dressing change. Preoperative bra size was 36DD. The distance from the jugular notch to the nipple was 25.5 cm on the right breast and 24.5 cm on the left breast. Postoperative bra size is 36C. The distance from the jugular notch to the nipple is 22 cm on each breast.
-
A 36-year-old patient, preoperative view. Bra size is 38D. The distance from the jugular notch to the nipple is 31.5 cm on each breast.
-
A 36-year-old patient, appearance 2 months after breast reduction by suction alone; 570 mL was removed from the right breast and 550 mL from the left breast. The distance from the jugular notch to the nipple is 28 cm on the right breast and 28 cm on the left breast. Preoperatively, bra size was 38D. The distance from the jugular notch to the nipple was 31.5 cm on each breast
-
A 36-year-old patient, preoperative lateral view. Bra size is 38D. The distance from the jugular notch to the nipple is 31.5 cm on each breast.
-
A 36-year-old patient, lateral view of the breast 2 months after breast reduction by suction alone; 570 mL was removed from the right breast and 550 mL from the left breast. The distance from the jugular notch to the nipple is 28 cm on the right breast and 28 cm on the left breast. Preoperatively, bra size was 38D. The distance from the jugular notch to the nipple was 31.5 cm on each breast
-
Female breast, anterior view.





