Practice Essentials
This article offers a detailed review of injuries of the thumb. The topics covered include the following:
-
Thumb phalangeal fractures
-
Mallet thumb
-
Thumb interphalangeal (IP) dislocations
-
Thumb metacarpophalangeal (MCP) dislocations
-
Thumb metacarpal fractures
-
Metacarpal head
-
Metacarpal shaft
-
Metacarpal base
-
Extra-articular fractures
-
Bennett fracture [1] (See the image below.)
-
-
Rolando fracture [2] (See the image below.)
-
-
Comminuted fractures
-
Thumb carpometacarpal (CMC) dislocations
-
Thumb MCP ulnar collateral ligament injuries (skier and/or gamekeeper thumb) [3]


Workup in thumb fractures and dislocations
Because the thumb lies out of the plane of the hand, suspected fractures and/or dislocations of the thumb may require special radiographic views.
In Robert view, the hand is hyperpronated so that the dorsum of the thumb lies on the radiographic plate; this gives a true anteroposterior view of the thumb. [4]
In Bett view, the hand is pronated approximately 20-30° and the imaging beam is directed obliquely at 15° in a distal to proximal direction, centered over the trapeziometacarpal joint. In this view, the thumb carpometacarpal (CMC) joint is well visualized, as well as the articulations of the trapezium with the trapezoid, scaphoid, and index metacarpal. [4]
Specific findings include the following:
-
Metacarpophalangeal (MCP) joint - Radiographic demonstration of a widened MCP joint suggests soft tissue interposition within the joint, indicating a possible irreducible dislocation [5]
-
Skier and/or gamekeeper thumb - Occasionally, a bony avulsion fracture from the base of the proximal phalanx is observed; palmar or radial subluxation of the proximal phalanx may also be present [6]
-
CMC joint - A lateral radiograph shows a V sign that is formed by the radial aspect of the trapeziometacarpal articulation; a broken V sign may indicate undetected CMC joint subluxation [7]
Management of thumb fractures and dislocations
Management options include the following:
-
Thumb phalangeal fractures - Fractures of the thumb phalanges have no distinct difference in treatment from fractures of phalanges of digits 2-5
-
Distal phalanx fractures - Tuft fractures rarely require reduction or fixation, while unstable shaft fractures may need percutaneous pinning longitudinally across the fracture and into the proximal phalangeal head
-
Proximal phalanx fractures - Splint nondisplaced fractures of the proximal phalanx for up to 4 weeks, followed by early motion; incongruous intra-articular fractures require reduction and fixation, and displaced fractures of the proximal phalanx may need operative intervention
-
Mallet thumb - Treatment for mallet thumb is usually nonoperative; follow full-time splinting in extension for 6 weeks (splint must be on at all times) by night splinting in extension for an additional 6-8 weeks
-
Thumb interphalangeal (IP) dislocations - Thumb IP dislocations generally are reduced easily in a closed fashion
-
Dorsal MCP dislocation - Attempt closed reduction in patients with thumb MCP dislocations regardless of the presence of radiographic or clinical signs of irreducible dislocation
-
Palmar MCP dislocation - A closed reduction should be performed and an assessment made of collateral ligament stability; an unsuccessful reduction or the presence of unstable collateral ligaments requires an open surgical approach
-
Thumb metacarpal fractures - Head fractures can be treated with open reduction and internal fixation (ORIF), while closed reduction can be attempted in deformed shaft fractures, and base fractures may be treatable with closed reduction or ORIF
-
Thumb CMC dislocations - These frequently reduce spontaneously, but for irreducible dislocations or unstable injuries, a surgical approach is indicated
-
Skier and/or gamekeeper thumb - Acute incomplete ruptures can be treated with a short arm thumb spica cast, while for acute complete injuries, surgery is generally recommended; chronic ruptures usually require reconstruction
For patient education resources, see the Breaks, Fractures, and Dislocations Center, as well as Broken Finger, Finger Dislocation, and Broken Hand.
History of the Procedure
Historically, these injuries have been treated with immobilization; even today, most can be treated nonoperatively. Surgical techniques of fixation were not developed until the early 20th century. [8] As fractures of the diaphysis of thumb metacarpal or phalanges may be allowed to heal with a greater degree of angular malunion than those fractures in the other fingers (due to the greater degree of mobility of the thumb), nonoperative treatment continues to be successful in appropriate cases. [4]
Problem
An opposable thumb was an integral development in the advancement of the human species and remains an important factor in functioning within today's technology-driven society. Thumb injury may lead to a high level of disability in a person's professional and personal life, leading to the loss or reduction of innumerable productive hours in the workplace as well as impairment in the patient's activities of daily living. Loss of use of thumb is a loss of 40% of hand function [9] , which is evaluated as 22% of the function of the body as a whole. [10]
Epidemiology
Frequency
In general, fractures of the hand occurred most frequently in the young adult age group. [11, 12] However, Stanton et al found that fractures of the thumb were most common in children and the elderly. [13] In children younger than 16 years, 22% of all metacarpal or phalangeal hand fractures occurred in the thumb; in those aged 17-40 years, only 12% of hand fractures occurred in the thumb; in those older than 65 years, the rate of thumb fracture rose again to 20% of all hand fractures. [13] In the elderly, the thumb was the most common tubular bone fractured in the hand, and fracture patterns were oblique and intra-articular. [13]
A literature review by Lehrman et al regarding hand or wrist injuries among professional athletes in sports such as baseball, football, boxing, and basketball found thumb collateral ligament injuries to be the second most common type of hand/wrist trauma (13.9%), after metacarpal fractures of the hand (34.5%). [14]
Etiology
Thumb injury results from both direct and indirect trauma. Injuries most frequently result from leisure activities on the weekend, with presentation often delayed. [12] Motor vehicle and bicycle accidents are the most common causes. [11]
Pathophysiology
Thumb phalangeal fractures
The thumb has only 2 phalanges: the distal and proximal phalanx. Fractures of these phalanges are generally diagnosed and treated identically to phalangeal fractures of the other digits.
Distal phalanx fractures can be separated into extra-articular tuft fractures and intra-articular tendon avulsion injuries. Tuft fractures generally are caused by a crush injury to the distal thumb. Tuft fractures frequently are associated with nail bed injuries and are technically open fractures when a nail bed injury is present. Tendon avulsion injuries are often secondary to avulsion of the extensor tendon at its terminal insertion into the distal phalanx. The tendon may pull off a fragment of bone resulting in a "bony" mallet thumb deformity. The flexor pollicis longus, in contrast to the finger flexors, also can be avulsed at the musculotendinous junction.
Proximal phalanx fractures consist of fractures of the phalangeal head and shaft. These are treated similarly to phalangeal fractures of digits 2-5, although the mobility of the thumb allows for more acceptance of angulation and rotation. [15]
Mallet thumb
Closed mallet thumb injuries are uncommon. The mechanism of closed injury is usually secondary to an acute forceful flexion of the thumb IP joint, leading to an avulsion of the extensor tendon with or without a bony fragment at its distal phalangeal insertion. The open injury secondary to laceration of the distal portion of the extensor tendon is more frequent.
Thumb IP dislocations
The IP joint of the thumb functions as a hinge (trochlear) joint with motion primarily in the plane of flexion and extension. Collateral and accessory collateral ligaments as well as the trochlear shape of the joint provide IP joint stability to radial and ulnar forces. The palmar plate, a thick fibrocartilaginous structure, provides support to the volar aspect of the joint. A flexible capsule is present dorsally and volarly providing freedom in flexion and extension. In approximately 70% of individuals, a single sesamoid is present within the palmar plate at the IP joint; this functions to increase mechanical advantage of the flexor pollicis longus (FPL) tendon.
IP joint dislocations, usually dorsal, occur infrequently. The mechanism of injury usually consists of hyperextension with a variable amount of rotation. An inability to reduce the dislocation may be secondary to interposition of the palmar plate, secondary to rupture of this structure. The ruptured palmar plate is subsequently trapped in the joint with the attempted reduction maneuver. Most reported irreducible dislocations are open with the base of the proximal phalanx exposed in the wound.
Thumb MCP dislocations
Dorsal dislocations are much more common than volar dislocations. Volar dislocations are rare and usually are associated with collateral ligament ruptures. Volar dislocations are more commonly irreducible than dorsal dislocations, secondary to interposition of the dorsal capsule and either the extensor pollicis longus (EPL) or the extensor pollicis brevis (EPB).
The mechanism of injury for dorsal dislocations consists of MCP joint hyperextension secondary to falling on an outstretched hand or axial loading to the tip of the thumb. Dorsal dislocation frequently leads to the palmar plate tearing proximally and moving distally. The palmar plate may become interposed within the joint, leading to an irreducible dislocation.
Thumb metacarpal fractures
Thumb metacarpal head fractures are rare secondary to mobility of the thumb CMC joint. Direct trauma to the joint is the usual mechanism of injury. Open reduction and internal fixation (ORIF) is indicated for displaced intra-articular injuries. Thumb metacarpal shaft fractures also are rare secondary to mobility of the thumb CMC joint. Because of stronger cortical bone of the thumb metacarpal, much higher energy is needed to fracture the thumb metacarpal shaft versus the metacarpal shafts of other digits. These fractures frequently result in shortening and malrotation. Shortening and collapse occur secondary to the lack of intermetacarpal ligaments and deforming forces of intrinsic musculature.
Thumb metacarpal base fractures are common. The mechanism of injury is usually an axial load applied to a slightly flexed metacarpal shaft. The thumb CMC joint has considerable mobility secondary to the bony anatomy of the trapezium and metacarpal base, two apposed saddles whose longitudinal axes are perpendicular to one another. Ligamentous stability at the trapeziometacarpal joint is maintained by the anterior (volar) and posterior oblique ligaments, anterior and posterior intermetacarpal ligaments, and the dorsal radial ligament. Thumb metacarpal base fractures are classified into extra-articular and intra-articular. Intra-articular fractures are more common and are subdivided into Bennett fractures, Rolando fractures, and comminuted fractures.
Extra-articular fractures at the base of the thumb metacarpal are common, are usually transverse or oblique, and occur at the proximal metaphyseal-diaphyseal junction. The distal fragment usually is adducted and flexed secondary to the pull of the adductor pollicis (AP), abductor pollicis brevis, and flexor pollicis brevis.
Bennett fracture (see first image below) is an intra-articular basilar fracture of the thumb metacarpal in which a single volar ulnar base portion remains intact. The anterior (volar) oblique ligament holds the volar ulnar fragment in place by its attachment to the trapezium. The remainder of the metacarpal shaft is displaced dorsally and radially secondary to the pull of the abductor pollicis longus (APL), AP, and thumb extensors (see second image below).
 The strong pull of the abductor pollicis longus frequently leads to displacement of the metacarpal shaft in a radial direction and may require operative intervention.
The strong pull of the abductor pollicis longus frequently leads to displacement of the metacarpal shaft in a radial direction and may require operative intervention.
A Rolando fracture (see image below) is a 3-part intra-articular basilar fracture of the trapeziometacarpal joint. In addition to the metacarpal shaft, a fracture configuration of a T or Y pattern with both volar and dorsal fragments is present. It is the least common of the metacarpal base fractures. The volar carpal ligament remains attached to the volar fragment, and the APL remains attached to the dorsal fragment.
Comminuted fractures are relatively common; they produce a pilon type of fracture as well as varying degrees of articular surface impaction. [16]
Thumb CMC dislocations
Thumb CMC dislocations are rare secondary to the strength of the volar (oblique) ligament, which usually produces an intra-articular avulsion fracture with a fragment attached to this ligament. Spontaneous reduction usually occurs in those rare instances in which a pure thumb CMC dislocation occurs. Ligamentous disruption may occur with this injury and may lead to long-term subluxation and painful hypermobility. [17, 18]
Thumb MCP ulnar collateral ligament injuries (skier and/or gamekeeper thumb)
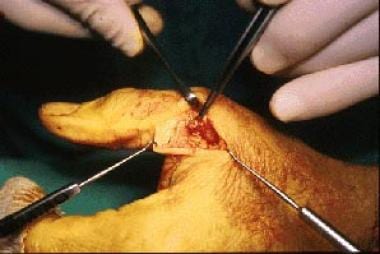
Thumb MCP ulnar collateral ligament injuries usually occur because of extreme valgus stress to the thumb. This may lead to complete or incomplete rupture of the thumb MCP ulnar collateral ligament. An incomplete rupture consists of rupture of the proper ulnar collateral ligament with the accessory collateral ligament remaining intact. Complete rupture consists of both the proper and accessory ulnar collateral ligaments. Rupture of the ulnar collateral ligament is usually from the distal insertion on the base of the proximal phalanx. A variation known as a Stener lesion (see the image below) results when this distal end comes to lie superficial and proximal to the adductor aponeurosis. This variant does not heal because the adductor aponeurosis is interposed between the proximal and distal ligament ends. [5, 3]
Presentation
Clinical presentation varies by location.
Thumb Phalangeal Fractures
Pain, swelling, decreased range of motion, and, occasionally, deformity are present in the fracture area. Distal phalangeal fractures may involve the nail bed. Carefully evaluate the sterile and germinal matrices if the nail bed is involved.
Mallet Thumb
Mallet thumb presents with the thumb in a slightly flexed posture and an inability to extend the thumb at the IP joint. These may be due to closed injury or an open laceration.
Thumb IP Dislocations
Thumb IP dislocations usually are dorsal and are easily recognized by the deformity created by the distal phalanx riding dorsal to the distal end of the proximal phalanx.
Thumb MCP Dislocations
Thumb MCP dislocations present with the usual findings of pain, swelling, and decreased motion in the area of the thumb MCP joint. The proximal phalanx may be hyperextended or parallel to the metacarpal in bayonet fashion. If a palmar dimpling, puckering, or abnormal skin crease is present, suspect an irreducible dislocation.
The proximal phalanx may be hyperextended and dorsal as well as parallel to the metacarpal. Radiographs show obvious dorsal dislocation of the proximal phalanx on the metacarpal. A widened joint space may indicate interposed soft tissues. Radiographic finding of the sesamoids interposed between the proximal phalanx and the metacarpal head indicates an irreducible dislocation by closed manipulation secondary to volar plate rupture and require surgical intervention.
Thumb Metacarpal Fractures
Metacarpal head
Fractures of the metacarpal head present with pain, swelling, decreased range of motion, and often are associated with soft tissue injury. Crepitus may be present with displaced intra-articular fractures.
Metacarpal shaft
Fractures of the metacarpal shaft present with pain, swelling, and often, angular deformity, typically apex dorsal or apex radial.
Metacarpal base
Patients with thumb metacarpal base fracture generally present with swelling, tenderness, limited range of motion, and occasionally an obvious deformity at the base of the thumb. Crepitus may be present with intra-articular fractures. The dorsally and radially displaced metacarpal shaft may be obvious on visual or manual inspection.
Thumb CMC Dislocations
Because these rare injuries frequently reduce spontaneously, the only acute findings may be pain, swelling, and decreased range of motion.
Thumb MCP Ulnar Collateral Ligament Injuries (Skier and/or Gamekeeper Thumb)
History of a valgus injury to the thumb is often present. This is a common injury in skiers who fall while continuing to hold onto their ski poles, producing an acute, forced radial deviation of the thumb. Pain, swelling, and ecchymosis over the ulnar aspect of the MCP joint are present. A mass or lump may present in the area of injury, representing the distal end of the torn ligament lying superficial to the adductor aponeurosis; this is referred to as a Stener lesion. Lack of a palpable mass does not exclude a Stener lesion. Obtain radiographs prior to valgus stress testing to exclude the presence of a thumb proximal phalanx or metacarpal fracture.
Perform valgus stress testing in both 30° of flexion and extension. Test the contralateral side for comparison with the injured side. If greater than 30° of laxity is present (or 15° of laxity greater than the noninvolved side) when giving a valgus stress in 30° of flexion, the proper ulnar collateral ligament is torn. If greater than 30° of laxity is present (or 15° of laxity greater than the noninvolved side) when giving a valgus stress in extension, the accessory ulnar collateral ligament is torn. If valgus stress testing reveals that both the accessory and proper collateral ligaments are torn, there is an approximately 80% likelihood of the presence of a Stener lesion. [19, 5]
Indications
Indications vary by location.
Thumb Phalangeal Fractures
Distal phalangeal fractures
Tuft fractures rarely require reduction or fixation. Transverse fractures of the distal phalanx may be unstable secondary to pull of the FPL on the proximal fragment. Unstable fractures may require percutaneous pinning.
Proximal phalangeal fractures
Incongruous intra-articular fractures require reduction and fixation. If there is more than 20-30° of angulation in the lateral plane, an IP joint extensor lag is produced and reduction is indicated. Less than 20° of angulation in the lateral plane may be acceptable. Displaced spiral or oblique fractures require accurate reduction and may be stabilized by percutaneous pinning or open reduction. Transverse fractures usually are stable after closed reduction.
Mallet Thumb
Treatment for mallet thumb is usually nonoperative. Continuous undisturbed splinting in extension for 6 weeks should be followed by night splinting in extension for an additional 6-8 weeks. Operative indications include open injury, failed closed treatment, chronic injury and/or mal-union, or a mallet thumb with bony avulsion.
Thumb IP Dislocations
Thumb IP dislocations generally are easily reduced in a closed manner. Operative indications include an irreducible dislocation or unstable IP joint after relocation, open injury, and chronic dislocations.
Thumb MCP Dislocations
Attempt closed reduction in all patients with thumb MCP dislocations, regardless of the presence of radiographic or clinical signs of irreducible dislocation. Operative indications are similar to those for thumb IP dislocations and include irreducible dislocation, unstable MCP joint after relocation, open injury, and chronic dislocations.
Thumb Metacarpal Fractures
Metacarpal head fractures
Treat metacarpal head fractures, intra-articular by definition, with ORIF if evidence of joint incongruity or displacement exists. Stable anatomic reduction allows for early motion and a reduced risk of post-traumatic stiffness and/or osteoarthritis.
Metacarpal shaft fractures
Shortening and collapse frequently occur secondary to the lack of intermetacarpal ligaments and the deforming forces of intrinsic muscles. Attempt closed reduction of displaced fractures. Malrotation is usually not a problem. Treatment goals are to restore length and preserve the web space. Indications for open reduction include shortening of more than 2 mm, angulation of greater than 20°, significant rotation, and open fractures.
Metacarpal base fractures
-
Extra-articular fractures: Closed reduction of extra-articular metacarpal base fractures usually are successful and can be maintained in a carefully applied thumb spica cast that excludes the distal phalanx. Transverse fractures generally are stable, while oblique fractures may displace after reduction with the metacarpal shaft going into adduction and flexion. Operative indications include angulation greater than 30°, comminuted fractures with shortening, and open fractures.
-
Bennett fracture: Closed reduction and thumb spica cast immobilization is effective in the treatment of Bennett fractures if reduction can be maintained. The strong pull of the APL frequently leads to displacement; thus, open or closed reduction with percutaneous pinning is frequently required (see image below). More than 1 mm of articular incongruity after closed reduction indicates operative intervention. This degree of articular incongruity is associated with an increased rate of articular degeneration in the thumb CMC joint.
-
Rolando fracture: The incidence of true Rolando fractures is low, thus assessing the importance of anatomic reduction on the long-term outcome of these fractures is difficult. It is complex to ascertain if the initial articular surface damage obtained with the original injury leads to degeneration at the CMC joint regardless of anatomic restoration of the joint. Treatment depends on the amount of articular incongruity and size of the fragments. An attempt at anatomic restoration of the joint surface is generally recommended. If the fracture is nondisplaced with articular incongruity less than 1 mm, percutaneous pin fixation may be attempted (see image below). Frequently, a single pin is inserted from the first metacarpal into the second metacarpal in an attempt to suspend the first metacarpal. More than 1 mm of incongruity requires assessment of piece size and either open reduction or distraction techniques. [20]
-
Comminuted fractures: Comminuted fractures of the thumb metacarpal base should be treated similar to Rolando fractures with small fragments (ie, distraction techniques). [21]


Thumb CMC Dislocations
Attempt closed reduction if necessary although these dislocations frequently reduce spontaneously. If the reduction is stable, then a thumb spica cast is the preferred treatment. Assess stability prior to thumb spica application. If the reduction is unstable, then percutaneous pinning or flexor carpi radialis (FCR) reconstruction is necessary. Open irreducible dislocations and treat with either pinning or FCR reconstruction.
Thumb MCP Ulnar Collateral Ligament Injuries (Skier and/or Gamekeeper Thumb)
Treat acute incomplete ruptures (in which the accessory collateral ligament remains intact) in a short arm thumb spica cast for 4 weeks. Surgical repair is recommended for acute complete ruptures or symptomatic chronic ruptures.
Relevant Anatomy
Bony anatomy
The thumb affords prehensile abilities that were essential in our evolution. The bony anatomy of the thumb consists of two phalanges and a metacarpal, which articulates with the trapezium bone in the distal carpal row. The metacarpal is actually a primordial phalanx.
MCP joint
The MCP joint has 6 degrees of freedom producing motion in planes of flexion and extension, abduction and adduction, and pronation and supination. The range of motion of the MCP joint of the thumb may be the most variable in the human body, depending upon individual variation in the radius of curvature of the metacarpal heads. Limited range of motion within this joint is associated with increased incidence of injury.
The MP joint has relatively little intrinsic stability. Lateral support arises from the proper and accessory collateral ligaments. The proper collateral ligament arises from the lateral condyles of the metacarpal and travels obliquely to insert on the volar aspect of the proximal phalanx. It is tight in flexion and loose in extension. The accessory collateral ligament arises from the metacarpal neck and inserts into the volar plate and the sesamoids. This structure is more volar in location than the proper collateral ligament and is tight in extension and loose in flexion.
CMC joint
The CMC joint consists of an articulation between the trapezium and the metacarpal base composed of two reciprocally interlocking saddles with perpendicular longitudinal axes. Ligamentous stability at the trapeziometacarpal joint is maintained by the anterior (volar) and posterior oblique ligaments, the anterior and posterior intermetacarpal ligaments, and the dorsal radial ligament. The anterior (volar) oblique originates on the trapezium and inserts into the volar beak of the thumb metacarpal. This is the most important ligament in maintaining CMC stability. The dorsal ligament is not as strong as the volar ligament but is reinforced by the APL.
Contraindications
No absolute contraindications to the treatment of thumb injuries exist. Virtually all injuries are amenable to immobilization or open reduction with or without fixation.
-
Bennett fracture.
-
Pinning of Bennett fracture.
-
Rolando fracture - There is intra-articular comminution.
-
Pinning of Rolando fracture.
-
An intraoperative photograph of a Stener lesion.
-
The strong pull of the abductor pollicis longus frequently leads to displacement of the metacarpal shaft in a radial direction and may require operative intervention.









