Practice Essentials
The zygomaticomaxillary complex (ZMC) is a functional and aesthetic unit of the facial skeleton. This complex serves as a bony barrier, separating the orbital constituents from the maxillary sinus and temporal fossa.
The zygoma has four bony attachments to the skull, and ZMC fractures are sometimes known as tetrapod fractures. Trauma to the ZMC can result in multiple fractures (ie, tetrapod), but solitary bony disruption may occur, as with isolated zygomatic arch fracture. This article focuses on the zygomatic arch fracture. [1, 2] For information on ZMC fractures, see the Medscape Drugs & Diseases article Zygomaticomaxillary Complex Fractures.
Workup in zygomatic arch fractures
As with most surgical patients, appropriate preoperative laboratory tests (eg, complete blood cell count, metabolic panels, activated partial thromboplastin time) and an international normalized ratio are necessary in those with zygomatic arch fracture.
A chest radiograph may be necessary before proceeding with the repair. Computed tomography (CT) scans have supplanted radiographs in the evaluation of midfacial trauma and are the current modality of choice. [3]
Magnetic resonance imaging (MRI) produces magnificently detailed images of the orbit. MRI enables multiplanar imaging and is excellent for evaluating soft tissue masses and optic nerve pathology. [4] However, although MRI provides exquisite detail of the orbital region, CT scanning remains the imaging modality of choice for evaluation of orbital trauma because of its ability to discern detail of bony structures.
Management of zygomatic arch fractures
Reconstruction of the zygomatic arch following injury is necessary for restoration of malar symmetry and support for the maxilla and masticatory loads. Repair of the zygomatic arch is usually performed in concert with repair of ZMC fracture stabilization.
Fractures of the zygomatic arch can be approached by various methods, including the following:
-
Direct cutaneous approach - The least invasive approach
-
Gillies approach
-
Hemicoronal approach - The most invasive approach, offering excellent visualization
-
Endoscopic approach
History of the Procedure
In 1751, Dupuytren detailed an intraoral and external technique to reduce a medial displaced zygomatic arch. Also described was an approach to the zygomatic arch by way of a plane between the temporalis muscle and deep temporalis fascia.
In 1844, Stroymeyer described the percutaneous traction technique that is still used for repair of zygomatic arch fractures.
In 1927, Gillies was first to mask incisions within the temporal hairline.
Epidemiology
Frequency
The zygoma is the second most commonly fractured facial bone, eclipsed in number only by nasal fractures. The vast majority of zygomatic fractures occur in men in their third decade of life.
In 1994, Covington et al reviewed 259 patients with zygoma fractures and found that ZMC fractures occurred in 78.8% of patients, isolated orbital rim fractures occurred in 10.8% of patients, and isolated arch fractures occurred in 10.4% of patients. [5] Of the isolated arch fractures, 59.3% were displaced or comminuted.
Etiology
Zygoma fractures usually result from high-impact trauma. Leading causes of fractures include assault, motor vehicle or motorcycle accidents, sports injuries, and falls.
A retrospective study by Cohn et al found that out of 218 patients with isolated zygomatic arch fractures, the most common injury source was assault (55%), while accidents were the least common (17.9%). [6]
Presentation
Arch fractures may result in trismus, flattening of the midface, asymmetry of the malar regions, or a reduction in oral aperture.
In the aforementioned study by Cohn et al, of 218 patients with isolated zygomatic arch fractures, the investigators found that compared with individuals who were managed conservatively, those who underwent surgery were more likely to have presented with zygomatic deformity (97.7% vs 18.4%), paresthesia (29.5% vs 2.9%), and trismus (29.5% vs 6.9%). [6]
Indications
Surgical exploration and fracture repair are indicated with a displaced or comminuted fracture, trismus, or significant aesthetic deformity.
Although rarely indicated, emergent surgical repair and decompression are necessary when exophthalmos or signs and symptoms of an orbital apex syndrome are present.
Relevant Anatomy
The zygomatic arch is a principal constituent of the midfacial skeleton, bound by the zygomaticotemporal suture line posteriorly and the malar eminence anteriorly. [7, 8]
The arch, in essence, is a rim of bony armor surrounding the temporalis muscle and the coronoid process of the mandible and is the origin of the masseter muscle.
The zygomatic arch is part of the facial subunit known as the zygomaticomaxillary complex (ZMC). The ZMC has 4 bony fusion sites with the skull.
See the image below.
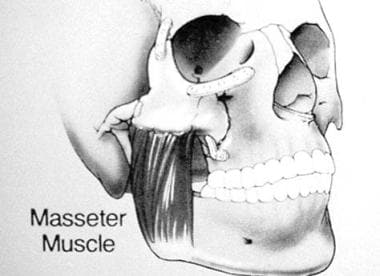 Anatomic depiction of the masseter muscle as it relates to the zygomaticomaxillary complex and mandible.
Anatomic depiction of the masseter muscle as it relates to the zygomaticomaxillary complex and mandible.
Contraindications
Surgical correction is contraindicated in patients who are medically unstable or unable to tolerate anesthesia.
-
Gillies approach to reduction of a zygomatic arch fracture.
-
Anatomic depiction of the masseter muscle as it relates to the zygomaticomaxillary complex and mandible.









