Practice Essentials
Capillary malformations are a form of vascular anomaly that present in patients at birth. Vascular anomalies make up a spectrum of disorders involving the endothelium and can be classified broadly into vascular tumors and vascular malformations. As elucidated by Mulliken and Glowacki, these categories, representing the only two major types of vascular birthmarks, reflect differences in clinical, histologic, hematologic, and radiologic/skeletal features. Their analysis of 49 specimens highlighted a number of key differentiating factors, with the histologic features considered to be the most important. Indeed, plump endothelia, increased mast cells, and multilaminated basement membranes characterize hemangiomas, while flat endothelia, normal mast cell numbers, and a thin basement membrane distinguish vascular malformations. [1] It is imperative to understand the key differences between these malformations in order to determine the most appropriate management. [1]
 A 12-year-old boy presenting with bluish discoloration of the right thenar eminence and index finger. The lesion has been present since birth and changes in size when he raises his arms or exercises strenuously. Upon physical examination, the mass is soft and rubbery. No palpable thrill or audible bruit is present.
A 12-year-old boy presenting with bluish discoloration of the right thenar eminence and index finger. The lesion has been present since birth and changes in size when he raises his arms or exercises strenuously. Upon physical examination, the mass is soft and rubbery. No palpable thrill or audible bruit is present.
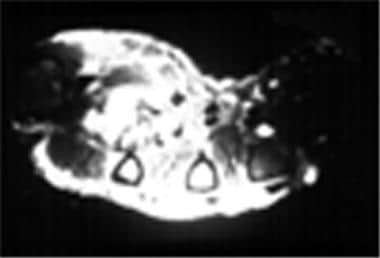 An image from an MRI study of the right hand of the patient in the image above, detailing the vascularity of the lesion.
An image from an MRI study of the right hand of the patient in the image above, detailing the vascularity of the lesion.
 Intraoperative view of the lesion in the first and second images shown above. Note the irregular mass of vessels that are adherent to the digital neurovascular bundles, tendons, and lumbrical muscle belly.
Intraoperative view of the lesion in the first and second images shown above. Note the irregular mass of vessels that are adherent to the digital neurovascular bundles, tendons, and lumbrical muscle belly.

Hemangiomas
Subsequent to Mulliken and Glowacki's report, Enjolas and Mulliken described congenital hemangiomas as separate from infantile hemangiomas, being present at birth (as opposed to infantile hemangiomas, which most commonly appear within the first month of life). They described two varieties: rapidly involuting congenital hemangiomas (RICH) and noninvoluting congenital hemangiomas (NICH). [2]
North et al highlighted the presence of human glucose transporter 1 (GLUT-1) isoform as a useful differentiating factor between infantile hemangiomas and other vascular anomalies. GLUT-1 is uniquely expressed on the endothelial cells of hemangiomas and is not seen in congenital hemangiomas (RICH, NICH), vascular malformations, pyogenic granulomas, or granulation tissue. [3] Leon-Villapalos et al confirmed these findings in a cohort of patients with vascular anomalies over a 7-year period and found 19 cases of juvenile/infantile hemangiomas, all but one positive for GLUT-1 expression; two cases of NICH that were negative for GLUT-1 expression; 29 cases of vascular malformations (8 capillary, 11 lymphatic, 7 venous, 3 arteriovenous), all negative for GLUT-1; and eight negative controls (4 pyogenic granulomas and 4 granulation tissue samples), all negative for GLUT-1. [4]
Vascular malformations
Vascular malformations result from faulty embryogenesis, resulting in structural and morphologic anomalies. Their appearance can fluctuate in response to changes in blood pressure gradients and flow, collateral formation development, shunting, and changes in hormonal status. [5] Most lesions are mixed, and the predominant vessel is used to describe the lesion. They are not considered neoplastic lesions and are commonly associated with skeletal deformities and hypertrophy. These lesions are commonly present at birth and grow proportionally as the child grows. They also grow with puberty, infection, or trauma and do not involute or regress. They tend to be difficult to remove, as the edges are diffuse and may infiltrate important nerves and vessels.
The natural history of the lesion is dictated by its hemodynamic and lymphodynamic characteristics, ie, whether the lesions are high (fast) flow or low (slow) flow. The low-flow group is composed of capillary malformations, venous malformations, and lymphatic malformations or a combination of these. High-flow lesions include arterial malformations and arteriovenous malformations and are typically associated with bruits, thrills, pulsations, and increased temperature. They expand with increased blood pressure/increased flow and secondary to trauma/surgery by collateral blood vessel formation. [1]
Epidemiology
Frequency
The prevalence at birth of capillary malformations is reported at 0.3% without predisposition to either sex.
Etiology
Genetic studies have mapped capillary malformations to chromosome 5q14-21, showing a defect in the RASA1 gene. The RASA1 gene encodes p120 Ras GTPase-activating protein. When mutated, p120 Ras GTPase-activating protein binds to Krev-1/rap1a, an integrin β1–mediated cell adhesion and angiogenesis protein. The pathogenesis of capillary malformations is not understood. [6]
Pathophysiology
Capillary malformations
Unlike a hemangioma, which is a vascular neoplasm, a port wine stain (which is technically an outdated term) is a capillary malformation with progressive dilation of superficial dermal vessels. It is almost always present at birth and appears equally among males and females.
Port wine stains appear mainly on the face and upper trunk but can also develop on the extremities. While 45% of facial port wine stains are contained in one dermatome, 55% cross over. [7] Lesions can vary in shade, depending on the underlying vessels (see the classification below), and grow in proportion to the growth of the child. Over time, if not treated, the lesions may become nodular, taking on a "cobblestone" appearance, and can also undergo hypertrophy, as can the surrounding soft tissue. [8] This may affect psychological well-being and personal development. [9]
Most port wine stains are clinically harmless but may be associated with Sturge-Weber, Klippel-Trenaunay, or Parkes-Weber syndrome. Periocular involvement can result in glaucoma, necessitating the need for treatment, and midline cephalic or spinal capillary malformations could indicate possible encephalocele or spinal dysraphism. [10, 11]
Wagner Classification [12] (Open Table in a new window)
Grade 1
|
Sparse, pale, nonconfluent discoloration |
Grade 2 |
Denser pink, nonconfluent discoloration |
Grade 3
|
Red, discrete, ectatic vessels |
Grade 4
|
Confluent patch |
Grade 5
|
Nodular lesion |
Prognosis
A literature review by van Raath et al looking at an approximately three-decade–long period starting in 1986 reported that treatment outcomes for port wine stains did not improve over these 30 years. The investigators found that 75-100% clearance was obtained in 21% of patients but that mean clearance did not demonstrate an upward trend over time. [13]
-
A 12-year-old boy presenting with bluish discoloration of the right thenar eminence and index finger. The lesion has been present since birth and changes in size when he raises his arms or exercises strenuously. Upon physical examination, the mass is soft and rubbery. No palpable thrill or audible bruit is present.
-
An image from an MRI study of the right hand of the patient in the image above, detailing the vascularity of the lesion.
-
Intraoperative view of the lesion in the first and second images shown above. Note the irregular mass of vessels that are adherent to the digital neurovascular bundles, tendons, and lumbrical muscle belly.
-
The excised specimen from the patient in the previous images.
Tables
Grade 1
|
Sparse, pale, nonconfluent discoloration |
Grade 2 |
Denser pink, nonconfluent discoloration |
Grade 3
|
Red, discrete, ectatic vessels |
Grade 4
|
Confluent patch |
Grade 5
|
Nodular lesion |





