Background
The pinna makes only a tiny contribution to the function of hearing. The main function of the pinna is to "look normal." Normal is, of course, a subjective judgment with a cultural bias. In Western society, popular comic cartoon characters often are endowed with large, prominent, or protruding ears. A child with prominent ears is often the target of invidious comparison to such characters and must carry the burden of an "unacceptable" evaluation from peers, a burden that may be carried into adulthood. The image below illustrates surgical correction of prominent ear.
 Concha-mastoid sutures. Left: preoperative view of 10-year-old boy in whom auricular prominence was caused by excessively deep conchal cups. Treatment was bilateral concha-mastoid sutures. Right: postoperative view.
Concha-mastoid sutures. Left: preoperative view of 10-year-old boy in whom auricular prominence was caused by excessively deep conchal cups. Treatment was bilateral concha-mastoid sutures. Right: postoperative view.
Despite recognized standards in idealized facial proportions and anthropomorphic measurements for each facial feature, societal standards change depending on which new fashion model is popular or which current figures are revered in today's media. Often, in this increasingly visual world, when wishing to depict the oddball character, the less intelligent individual, and the funny looking kid, the media often select subjects with large, prominent, or oddly shaped ears. These subjects are initially assigned a level of immaturity or low intellect. The fact remains that, without calipers or other instruments of measure and without memorizing a set of standards, humans visually understand when facial features appear in balance, and few, if any, features elicit such negative responses as ears that are prominent, overly large, or misshapen. [1, 2] Unfortunately, these individuals are often assigned many of the above negative traits.
History of the Procedure
Ely is credited with the first otoplasty in 1881. At the turn of the century, Morestin expanded on Ely's technique with ingenuity. He described concha-mastoid (C-M) sutures, antihelix (Mustardé) sutures, an antihelix incision, and thinning of the posterior surface of the cartilage. Morestin's article appeared in an orthopedic journal in 1903 and contained only a single drawing, thus it was overlooked in subsequent decades. In a 1910 publication, Luckett dealt with the flat antihelix by incising the cartilage and creating a crest by joining the cut edges with mattress sutures.
In a 1930 article, GW Pierce reported weakening the line of the crest of the antihelix by scoring the posterior surface of the cartilage, facilitating the formation of the fold. Gibson in 1958 demonstrated that disruption of a balanced cross-section of costal cartilage caused warping away from the site of disruption. Stenstrom studied cross-sections of scored auricular cartilage while working with Pierce. He noted that the cartilage curled away from the scored surface, following Gibson's principle; therefore, he replaced posterior scoring with anterior scoring of the antihelix. [3] Converse and Tanzer made parallel cartilage incisions, which were joined to form a tubelike crest. [4] Mustardé employed mattress sutures to create the fold of the antihelix. [5, 6] Morestin's C-M sutures for reducing the deep concha were redescribed by Furnas in a 1978 article. Elliott and Gault added improvements. [7, 8]
Anterior approaches for altering the antihelix were described by J Davis in 1978 and by Kaye in 1967. Nordzell and Erol described recent modifications of the anterior approach. [9, 10] More recently, the authors have stressed the importance of conchal enlargement on overall ear structure and prominence.
Problem
Essentially, all current otoplasties are effective in reducing the prominence of the ear; however, one technique may be better than another for a special problem and each technique is characterized by certain incidental changes in the nature or the shape of the auricle. For the most part, these incidental changes are an acceptable exchange.
An ear appears prominent or protruding if it projects more than 15-20 mm or more than 21-30° from the temporomastoid plane of the skull. The mean length of the ear (sa-sba, ie, superaurale to subaurale) in boys is 55 mm when aged 6 years, 60 mm when aged 12 years, and 62 mm when aged 18 years. In girls, the values are 54 mm, 58 mm, and 58 mm at ages 6, 12, and 18 years, respectively. The mean width of the ear (pra-pa, ie, preaurale to postaurale) is 34 mm, 35 mm, and 36 mm in boys and 33 mm, 34 mm, and 34 mm in girls at ages 6, 12, and 18 years, respectively. One standard deviation in width is 2.0-2.5 mm and in length is 3.0-3.5 mm. An ear that is 2 or more standard deviations from the mean is viewed as abnormally large (macrotia). Excessive projection is a far more frequent problem than excessive size.
Indications
The first step in assessing the patient for otoplasty is determining the anatomic causes of protrusion of the ear. The most common causes of protrusion of the external ear are (1) underdevelopment or effacement of the antihelix, (2) overdevelopment of the deep concha, or (3) a combination of both of these features.
Contributing features that accentuate auricular protrusion are (1) prominence of the mastoid process, (2) protrusion of the lower auricular pole (ie, cauda helicis, lobule, cavum concha), and (3) a prominent tipped upper auricular pole. Cranial deformity as in uncorrected positional plagiocephaly can significantly affect ear position and prominence.
Auricular protrusion may be one element of a more complex auricular deformity such as a constricted ear, Stahl ear (third crus), macrotia, or syndromic facial deformity.
True macrotia is rare. It can be seen in association with vascular malformations, hemihypertrophy, neurofibromatosis, and secondary to hemangioma. It is more obvious if the ear is prominent; the above otoplasty methods apply in mild macrotia. If the ear is so large as to be truly conspicuous, the Antia-Buch technique and its variations provide true reduction of the ear with minimal aesthetic compromise.
This article discusses the evolution of current technique for correction of the prominent ear and demonstrates how the technique has been modified to correct a wide variety of deformities from simple ear prominence to those with accompanying deformation of the helical rim, excessive prominence of the lobule, and moderate degrees of constriction. Inherent in the technique is an understanding of the proper balancing and subtle positioning of the varied ear contours to obtain an outcome that has a satisfactory appearance and that does not immediately appear to have been operated on. While the final ear position and shape are critical, the exact measurements are not.
Many of the patients presenting for otoplasty have visibly prominent ears, but not all people with large and prominent ears have a desire to change their appearance, and many, even if teased in childhood, have become comfortable with their appearance. That being said, experience has demonstrated that many of the parents bringing their children in for prominent ear correction are strongly motivated by the desire to spare their child the embarrassment and teasing that they endured. Parents may subsequently elect to undergo otoplasty after their child has had surgery. In these cases, satisfaction and feelings of relief are constant features of their recovery.
These issues are important when deciding the appropriate timing for the surgery, and whether the decision to operate should be made based on the parents' concerns or should wait until the child expresses these concerns. This is a decision that needs to be made on a case-by-case basis. However, by the time children approach 5 years of age, they may have been teased, even if the teasing has not started to affect the way they feel about themselves. Once the discussion ensues, they express their willingness to go through the surgery to avoid this teasing.
Children younger than 5 years of age are rarely perceptive enough about their appearance or comments made about them to feel that surgery is urgent. Likewise, experience has demonstrated that these younger children may have significant difficulty cooperating with the postoperative routines (ie, dressings and activity limitations). Taken together, with very rare exception, age 5 years is the low end of the spectrum of patient age.
More subtle cases of ear prominence, distortion of ear shape, or ear asymmetry may not spark the desire for correction until a child is older, more concerned about overall appearance, or eager to adopt a different style and wear his or her hair back or cut short. In each case, the ear or ears that may have been hidden are now exposed.
There are very few contraindications for otoplasty. In the pediatric population, surgery is appropriate and extremely well tolerated provided that the child does not strongly resist the idea of surgery. If a child begins to misbehave or becomes excessively worried about even going to the doctor for a preoperative discussion or going to the hospital, it is best to delay the surgery until the child openly requests the procedure. Another contraindication is a history of chronic ear infections and ear drainage that has not been thoroughly investigated and corrected. It is not uncommon for kids to have previously had myringotomy and pressure equalizer (PE) tube placement. If there is no active infection or significant drainage, then otoplasty can be performed safely.
At the other end of the age spectrum, adults seeking changes in ear shape, size, or prominence must, as with any aesthetic surgery candidate, be able to express their reasons for seeking a change at this stage and demonstrate realistic expectations of what the change is going to mean for them. Careful case selection is critical and is never more important than when the deformity is a minimal or subtle one. While beyond the scope of this article, the same careful case selection is important in patients who have previously undergone one otoplasty and are dissatisfied with the outcome.
In a 1978 article, Macgregor speaks of the "exquisite cruelty of young children toward the child who happens to look 'different.'" [11] These pediatric patients are highly motivated and cooperative. A truly gratifying psychological response to a well-performed otoplasty generally occurs. [12, 13] These children do not seek perfection in their otoplasties, but the surgeon must be aware that the occasional parent and/or caregiver has unrealistic expectations. A frank discussion about the operation and what it can achieve is in order, including the adverse effects, risks of surgery, and risks of anesthesia. Adolescent and adult patients often relate a history of embarrassment about their prominent ears from childhood years, but circumstances have precluded corrective surgery. These patients also are likely to be highly satisfied with the results of surgery.
Asymmetric features of the ears should be called to the attention of the patient and parents and/or caregivers, and a distinction should be made between features that are likely to be improved by surgery and those that will stay the same. The postoperative evaluation of the otoplasty by patient, family, and friends is inevitably more detailed than any preoperative evaluation.
Ethnic and cultural considerations may enter the algorithm. Prominent ears are typical among Celtic people, and in Japan, prominent ears are said to denote intelligence. However, it usually does not take long for children to conform to the cultural values of their adopted country. [14]
Relevant Anatomy
While the majority of otoplasty techniques have historically concentrated on the effaced antihelical fold as the main cause of ear prominence, failure to fully appreciate all the elements distorting the ear position and shape is a recipe for an unfavorable outcome. Experience has revealed that the vast majority of prominent ears demonstrate some degree of conchal hypertrophy, and the concha may be the cornerstone of the treatment of the prominent ear.
Correct analysis of each deformity is the most important step in otoplasty. Ear prominence results from one or more of the following features: 1) effacement or deficient antihelical fold, 2) conchal hypertrophy or abnormalities in conchal shape, 3) deformity of the underlying skeletal anatomy, and 4) macrotia, or generalized overgrowth of the ear. The first 2 of these features are accentuated when seen in combination with the decreased radius of the curve of the helical rim in the constricted ear.
The anterior (lateral) surface of the ear is the traditional reference plane for the anatomic nomenclature of the ear. However, many steps in an otoplasty, such as placing cartilage sutures, removing soft tissue, or trimming cartilage, may be performed on the posterior (medial) surface of the ear. From a posterior perspective, the concha and the fossa are viewed as eminences, and the crura are seen as grooves.
On cursory inspection, the shape of the cartilage framework appears to duplicate the visible ear. However, on closer examination, the auricular cartilage proves to be an incomplete skeleton with gaps, drop-offs, and irregularities in thickness, augmented with connective tissue and muscle. The surgeon must be facile in integrating these hidden features and illusions into his or her thought model of the patient's auricular anatomy. The images below illustrate auricular anatomy.
 Anatomy of auricular cartilage, anterior (lateral) and posterior (medial) surfaces. Although anterior landmarks are most familiar, posterior auricular landmarks are of special importance in otoplasty.
Anatomy of auricular cartilage, anterior (lateral) and posterior (medial) surfaces. Although anterior landmarks are most familiar, posterior auricular landmarks are of special importance in otoplasty.
The qualities of the auricular cartilage as a material and its biomechanical responses to external and internal forces must be assessed preoperatively, intraoperatively, and through the early postoperative period. Whether the auricular cartilage is made up of limber, stiff, or floppy cartilage is of prime importance in choosing the appropriate operative steps.
Cephaloauricular and scaphoconchal angles
Da Silva Freitas et al compared the cephaloauricular and scaphoconchal angles of 15 patients with prominent ears with 15 persons in a control group. The average of cephaloauricular angle was 47.7 degrees for the study group and 31.1 degrees for the control group. The average scaphoconchal angle was 132.6 degrees for the study group and 106.7 degrees for the control group. They concluded that measuring both angles may help in diagnosis of protruding ears. [15]
Antihelix
The antihelix normally forms a symmetric Y in which the gently rolled or folded crest of the root of the antihelix continues upward as the superior crus. The inferior crus branches forward from the root as a folded ridge. The root of the inferior crus of the antihelix sharply defines the rim of the concha. The inferior crus also forms the wall that separates the concha from the triangular fossa. The root and superior crus of the antihelix form the anterior wall of the scaphoid fossa, and the helix forms the posterior wall. The triangular fossa dips within the Y arms of the superior and inferior crura.
The corrugated contours of these auricular crests and valleys provide a pillar effect that stabilizes the pinna. The vertical walls of the conchal cup are translated to a semihorizontal plane as the concha merges with the folded crest of the antihelix. The scapha-helix is nearly parallel to the plane of the temporal surface of the head. If the roll of the antihelix and its crest are effaced and flat, rather than rolled or folded, the steep pitch of the conchal wall continues into the unformed antihelix and scapha and ends at the helix with little interruption. This places the scapha-helix complex nearly perpendicular to the temporal plane of the head, and the ear appears prominent. Such an ear also lacks the stability provided by the pillar effect and allows the superior auricular pole to protrude.
The literature has described effacement or deficiency of the antihelical fold as ranking foremost in most discussions of the prominent ear. This deformity manifests as a spectrum from a totally indistinguishable antihelix, with a confluent concavity from antihelix to scapha and the helical rim projected outward and forward, to loss of definition of only the superior antihelix with prominence of the upper pole of the ear.
Concha
The concha is an irregular hemispheric bowl with a defined rim. The normal scapha-helix surrounds the posterior part of the bowl as the brim of an inverted hat surrounds the crown. The pitch at which the scapha-helix projects from the conchal cup is determined by (1) the acuteness of the fold of the crest of the antihelix, (2) the height of the posterior wall of the conchal bowl, and (3) the completeness of the partial sphere formed by the concha.
If the posterior wall of the concha is excessively high and the concha is excessively spherical, then the angle and the distance between the plane of the scapha-helix and the plane of the temporal surface of the head are excessive. Usually such protrusion is distributed evenly around the posterior conchal wall. However, the cephalad part of the concha can protrude disproportionately, another cause for a protruding upper pole. Similarly, the caudal part of the concha can project disproportionately and cause a protruding lower auricular pole. These features require special attention in the operating room.
While less attention has been directed toward the importance of the concha in overall shape and projection of the ear, consider the 3-tiered configuration of the auricular cartilage framework. The more delicate antihelix and helical complex are mounted on the sturdier concha such that changes in conchal size and shape profoundly influence the overlying tiers. Bauer describes that it is rare to see prominence of the ear that does not have a conchal element.
The concha affects the prominence of the ear in 3 ways. These include 1) overall enlargement of the concha projects the ear away from the mastoid surface, 2) an extension of the helical crus across the concha creates a firm cartilage bar that pushes the ear outward, and 3) the effect of the angulation of the cartilage at the junction between the cavum concha; the sweep of cartilage up to the antitragal prominence affects the position and prominence of the lobule and lower third of the ear. The first of these is well recognized. Little attention has been drawn to the second, but once seen, it is easy to understand. Understanding the third element leads to understanding the approach to the isolated lower pole and lobule prominence.
The latter feature of conchal shape, while not the only cause of prominence of the lobule, appears to play a key role. As the cartilage angle between the concha cavum and antitragus becomes more acute (ie, as the antitragus tips closer toward the concha), this supporting structure projects the lower third of the ear and lobule outward. This feature has a greater influence on the lobule position than the commonly described helical tail.
A literature review by Mogl et al indicated that conchal hypertrophy can reliably be corrected via otoplasty using conchal excision. The investigators found no evidence that in such procedures a posterior approach to the concha in which the skin excision is separated from the cartilage excision is better than an anterior approach or vice versa. The literature also indicated that following resection, satisfactory results can be achieved either by approximating the cartilage edges using cartilage sutures or by allowing the edges to collapse spontaneously. [16]
Combination of protruding antihelix and concha
The combined effect of an effaced antihelix and a deep concha is also additive, causing a severe auricular protrusion.
Protruding mastoid process
A prominent mastoid process tends to push the concha forward, causing auricular prominence. Furnas has reported marked auricular protrusion caused by a dermoid cyst in the recess between the mastoid process and the concha. Removal of the cyst corrected the problem.
Although the effect of the underlying skeleton on ear prominence has had little attention, it should be recognized and taken into account in planning correction of the prominent ear. The external ear is mounted upon the bony base of the underlying temporal bone. Anomalies in skeletal shape and skeletal asymmetries can affect one or both ears. Perhaps the most recognizable example of this relationship is the change in ear position and projection in association with positional, nonsynostotic plagiocephaly. With the parallelogram deformation of the cranial vault, the ear on the side of occipital plagiocephaly is projected forward and is often more prominent.
In more subtle cases of this deformity, the ear prominence may become more evident in an older patient, in whom the ears are asymmetrically positioned and residual occipital flattening and mild facial asymmetry may not be readily apparent on first view. This effect of head shape on ear position is clear when viewing illustrations of Ely's description of his otoplasty technique in 1881.
A less subtle example of the influence of the skeleton on ear position is the effect of deficient temporal bone and medial positioning of the temporomandibular joint in hemifacial microsomia. In more severely affected cases, seen without microtia, the normal ear may seem to be sheared off the head, with the upper half of the ear projecting outward and the lower half canted medially toward the hypoplastic face. An additional example with some similarities occurs when the general craniofacial shape includes a relatively broad head, with a narrow face and mandible. Seen from the frontal view, there is a triangular configuration to the head and face. This slope from head to face may project the upper ear outward, creating the ear prominence but with otherwise normal features proportional to the ear.
Protruding cauda helicis
The cauda helicis is bound to the fibrofatty tissues of the earlobe by a network of connective tissue. The cauda helicis, which projects outward from the concha, carries the earlobe with it, causing it to protrude. This contributes to prominence of the lower pole.
Protruding earlobe
Some earlobes are not only large and pendulous but also are prominent due to the structure and form of the dense interlacing connective tissue fibers that shape the earlobe independent of the cauda helicis.
Soft tissues
The auricularis posterior attaches superficially to the ponticulus of the conchal cartilage and the posterior auricular ligament and most often consists of 2 bellies. This muscle is surrounded by fibroareolar tissue. Deep to the muscles and within the areolar tissue, small branches of the postauricular vessels and fine rami of the greater auricular nerve are found. Deep to these structures lie the mastoid fascia and the tendinous origin of the sternomastoid muscle.
Contraindications
The surgeon must be alert for the occasional adult who magnifies the severity of a small defect or who sees serious deformity in ears that others would judge as normal.
The authors prefer that a child considering surgery be at an age of awareness of his or her prominent ears and want them corrected. If parents are anxious to correct the child's prominent ears at an earlier age, the authors tend to defer surgery until later, although exceptions are made. Furnas has performed an otoplasty in an infant concomitant to correcting the webbed neck of a patient with Turner syndrome. Repeat otoplasty was performed when the patient was older. This likelihood of an incomplete correction or need for recurrent surgery speaks against early intervention except in rare cases.
An important step in gaining patient satisfaction is development of an individual surgical strategy that provides an excellent result for that patient. This starts with careful assessment of the defect.
Chronic otitis media, otitis externa, or conditions such as scalp infections or acne must be treated well in advance of surgery. A simple surgical wound infection can lead to an ear-threatening chondritis.
-
Mustarde sutures. Left top and bottom: Preoperative views of 10-year-old patient with absent antihelix root and superior crus, which caused prominence of each ear. Repositioning with Mustarde sutures corrected prominence and mild overhang of rim of helix. Right top and bottom: postoperative views.
-
Concha-mastoid sutures. Left: preoperative view of 10-year-old boy in whom auricular prominence was caused by excessively deep conchal cups. Treatment was bilateral concha-mastoid sutures. Right: postoperative view.
-
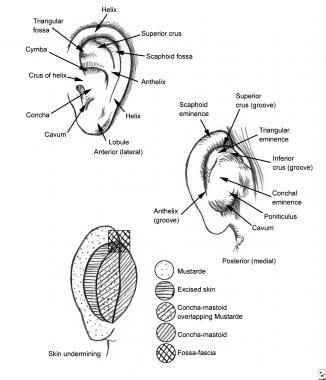
Surface anatomy of auricle (top, middle) and areas of skin undermining (bottom).
-
Anatomy of auricular cartilage, anterior (lateral) and posterior (medial) surfaces. Although anterior landmarks are most familiar, posterior auricular landmarks are of special importance in otoplasty.
-
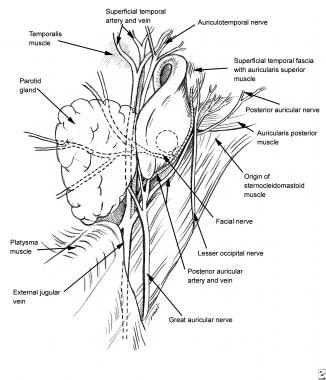
Anatomy of auricular vessels, nerves, and muscles.
-
Stiff, heavy cartilage. If cartilage is not limber and is resistant to force of sutures, the surgeon can choose from among additional steps that provide compliance. To reduce deep concha, cartilage may be excised from either a posterior (partial thickness or full thickness) approach or an anterior approach. Folding of the antihelix is enhanced by Stenstrom scoring; convexity of cartilage is produced by scoring one side of the cartilage, which releases interlocked stresses that curl cartilage in the opposite direction.
-
Left: Stenstrom scoring has been performed with No. 15 blade (in line with arrows) to augment camber of underdeveloped antihelix. Abrasion of antihelix is performed with unmounted, hand-held diamond burr (Midas B3D or B3D) via subcutaneous tunnel. Right: acrylic ear model.
-
Fossa-fascia sutures reduce prominence of upper pole of auricle. Deep temporal fascia is exposed by spreading the fibers of the auricularis superior and the superficial temporal fascia. Sutures pass from the deep temporal fascia to the cartilage of the scaphoid fossa or triangular fossa.
-
Mustarde (scapha-concha) sutures produce or increase the antihelix fold when the fold is absent or underdeveloped. Sutures bowstring from the scaphoid fossa or triangular fossa to the posterior conchal wall. In Kaye's modification, sutures are placed from the anterior approach through tiny incisions.
-
Concha-mastoid sutures and conchal nest. Sutures reduce excessive conchal projection, passing from the conchal cartilage to the mastoid fascia and to the aponeurotic fibers of the origin of the sternocleidomastoid muscle. Sutures flatten the conchal bowl against the mastoid process. Displacement or removal of excess soft tissues provides easier identification of the mastoid fascia and contributes to reduction of conchal projection.
-
Lobe sutures diminish prominence of projecting earlobe.