Background
The appearance of the brow is invested with an emotional, expressive, and psychological significance that makes it one of the most prominent features of the face. As the brow naturally descends with aging, its position often imparts undesired characteristics to the face, such as fatigue, sadness, anger, ennui, or other qualities that do not represent the individual's state of mind.
Many techniques have been developed to address the ptotic brow, and they are thoroughly reviewed in the following articles:
This article focuses on the plastic and reconstructive surgical considerations of the direct brow lift, which involves an incision (and the resulting scar) immediately over the eyebrows. Direct brow lift has become the most common approach to address the ptotic brow in Asian patients. However, although direct brow lift remains an excellent option for functional improvement, its popularity as a cosmetic technique has waned in the United States, having been replaced by more aesthetically satisfying methods that raise the forehead and the brow. A retrospective review performed by Rohrich et al that included 159 patients who underwent a brow rejuvenation procedure found that direct brow lift was performed in only 1.9% of the individuals; the endoscopic approach was the most common procedure, being carried out in 44.7% of patients. [1, 2]
As indicated above, the direct brow lift remains useful in certain clinical situations for functional restoration of the overhanging brow; this is the case, for example, in persons who are not candidates for more modern forehead-lifting techniques, who have thick eyebrows, who demonstrate asymmetries, and who are bald or have a high anterior hairline. [3] A study by Pascali et al of 50 consecutive male patients who underwent direct brow lift (along with upper blepharoplasty) found at 12-month follow-up that 98% of patients demonstrated statistically significant brow elevation. The investigators concluded that direct brow lift provides beneficial, long-lasting outcomes in bald men, in patients with a high anterior hairline, and in those in whom an asymmetry needs correction. The report states that the procedure is safe and replicable, with a short recovery period. Moreover, because this method requires no width dissection, it is less traumatic and can be rapidly performed, offering an advantage for elderly patients. [4, 3]
History of the Procedure
In 1919, Raymond Passot described excision of the skin and soft tissue above the eyebrows to eliminate wrinkles around the lateral eyes and above the brow. In the ensuing decades, the entire forehead became the focus of rhytidectomy, and various placements of incisions and degrees of undermining within the forehead and scalp were proposed. The early techniques did not produce long-lasting results until it was determined, in the 1950s, that incision of the frontalis muscle was required. [5] Modern bicoronal, endoscopic, and other techniques, in which incisions are placed in hidden areas, have eclipsed the direct brow excision in popularity.
Problem
Brow ptosis begins as early as the fourth decade of life. It contributes to sagging of the upper eyelid and most often imparts an aged, sad, and tired appearance to the face. Significant upper eyelid hooding may encroach upon the upper visual fields. Brow ptosis and resultant blepharoptosis generates compensatory activity of the frontalis muscle, which, over time, can create horizontal rhytides across the forehead and may contribute to ocular fatigue and headaches. The brow may descend to below the level of the supraorbital ridges.
No single ideal brow appearance is applicable for all patients. Women generally desire thin brows that lie slightly above the supraorbital ridge, with the apex of the arch lateral to the mid pupil. Men typically desire brows that lie at the level of the supraorbital rim and that are less arched. Ethnic variations in desired brow position and shape also must be considered when planning surgery for brow ptosis. [6]
Epidemiology
Frequency
According to the American Society of Plastic Surgeons, board-certified specialists performed an estimated 88,675 forehead lifts in 2020. This represented a 27% decrease compared with the 120,971 forehead lifts performed in 2000. [7] We hypothesize that the decline in brow surgery may be due to the rise in popularity of neurotoxin treatments.
Etiology
The main etiologic factors in brow ptosis are aging of the skin and gravity. As an individual grows older, the skin of the face loses tone, owing to a diminution in the amount of elastic fibers, glycosaminoglycans, and collagen. Loss of underlying fascial and muscle support also occurs, and opposition to the forces of gravity is diminished. Because the lateral brow has fewer attachments to the periosteum and has no underlying frontalis muscle, it usually descends more than the medial brow. [8]
Pathophysiology
See Etiology.
Presentation
Patients typically present with concerns related to a facial appearance that is aged, tired, or sad. Lateral support is reduced, and more ptosis develops in the lateral brow than in the medial area.
Functional sequelae of brow ptosis, such as deficits in the visual field, headaches, or ocular fatigue, are less common.
For excellent patient education resources, see eMedicineHealth's patient education article BOTOX® Injections.
Indications
Major reasons for performing a direct brow lift include (1) improvement in a visual-field deficit caused by overhanging eyebrow skin, (2) relief of ocular fatigue caused by compensatory overactivity of the frontalis muscle, (3) improvement in cosmetic appearance, and (4) requirement for a simple, expedient procedure. The cosmetic indication is tempered by the creation of scars above the eyebrows. This may be a secondary consideration for patients with marked brow asymmetry after previous traumatic injury or acquired facial paralysis.
Direct brow excision is best used in middle-aged or older men with male-pattern baldness, thick eyebrows, and lateral hooding, as depicted in the image below. [9]
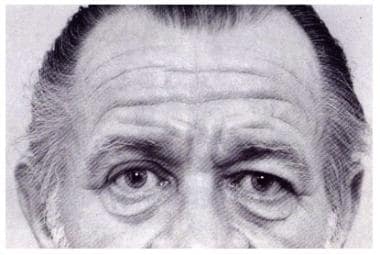 Direct brow lift. Typical patient for direct brow excision (McKinney, 1991). Courtesy of Springer-Verlag. Used with permission.
Direct brow lift. Typical patient for direct brow excision (McKinney, 1991). Courtesy of Springer-Verlag. Used with permission.
Patients who use a thick brow pencil to create the brow also may be candidates because they can conceal the scar with makeup. Scarring may be more obvious in patients with fair-colored eyebrow hair.
Specific physical findings that can be better addressed by other methods of brow lifting include ptosis of the forehead and medial eyebrows, transverse forehead wrinkles, vertical glabellar frown lines, transverse wrinkles at the root of the nose that become exaggerated when the forehead is manually depressed, and a drooping nose.
Relevant Anatomy
The tissue layers of the forehead include the skin, subcutaneous tissue, superficial galea, frontalis muscle, deep galea, loose areolar tissue, and periosteum. The forehead component of the superficial musculoaponeurotic system is the frontalis muscle with its galeal sleeve. The direct brow lift is an open technique with dissection in a plane superficial to the frontalis and orbicularis muscles, whereas in the bicoronal, midforehead, and endoscopic techniques, the dissection is performed in a subcutaneous, subgaleal, or subperiosteal layer. [10, 11, 12, 13]
The primary elevators of the brow are the paired frontalis muscles. They are vertically oriented and originate from the epicranial galea at the level of the anterior hairline, cover most of the forehead, and insert into the dermis of the lower forehead skin. The main eyebrow depressors are the corrugator supercilii, procerus, and orbicularis oculi muscles. [8]
The three nerves on each side of the forehead that are preserved during a direct brow lift are the (1) supraorbital nerve, (2) supratrochlear nerve, and (3) temporal (frontal) branch of the facial nerve. The supratrochlear nerve traverses the most medial aspect of the supraorbital rim (approximately 1.5 cm from midline) and innervates the ipsilateral corrugator muscle. The nerve travels through the corrugator and is easily cut when the muscle is sectioned to treat frown lines. [14]
The supraorbital nerve travels somewhat more laterally over the medial supraorbital rim (approximately 2.5 cm from midline) and divides into two branches. The deep branch travels laterally and then superiorly to reach the central frontoparietal scalp and vertex, coursing in a plane between the periosteum and the galea. The superficial branch of the supraorbital nerve divides several times and innervates the central forehead and hairline, coursing through and across the anterior aspect of the frontalis. Both the supraorbital and supratrochlear nerves can be damaged when they leave their bony foramina, where they are more adherent and less easily moved or stretched. [15, 16, 14] See the image below.
 Direct brow lift. Innervation by the supraorbital and supratrochlear nerves (Seckel, 1994). Courtesy of Quality Medical Publishing. Used with permission.
Direct brow lift. Innervation by the supraorbital and supratrochlear nerves (Seckel, 1994). Courtesy of Quality Medical Publishing. Used with permission.
The temporal (frontal) branches of the facial nerve enter the forehead within 2 cm of the lateral orbital rim, traveling just under the temporoparietal fascia to enter the frontalis muscle laterally; however, one cadaver study found the nerve to course as high as 4 cm above the lateral canthus. [17, 18]
The limited dissection of the direct brow lift avoids the supraorbital and supratrochlear nerves, although removing too much subcutaneous tissue laterally can injure the frontal branch of the facial nerve.
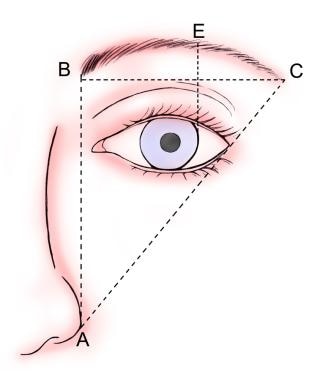
While the ideal brow position varies depending on sex and ethnicity, Ellenbogen and Westmore described general criteria for eyebrow position and contour that are helpful when planning and performing the brow lift. [19] See the image below, which corresponds to the following:
See the list below:
-
The brow should begin medially at a vertical line extending from the ipsilateral alar base and medial canthus (line A-B).
-
The brow should end laterally at an oblique line extending through the ipsilateral alar base and lateral canthus (line A-C).
-
The medial and lateral ends of the eyebrow should lie at approximately the same horizontal level (line B-C).
-
The apex of the brow should lie directly above the lateral limbus of the eye (line E).
-
The brow should arch above the supraorbital rim in women and lie approximately at the level of the rim in men.
These criteria are easier to meet with the direct brow lift than with other procedures because the brow can be precisely positioned on the forehead. [20]
For more information about the relevant anatomy, see Forehead Anatomy and Facial Nerve Anatomy.
Contraindications
Patients who cannot tolerate a scar above the eyebrow are not candidates for the procedure. Inadequate upper eyelid skin is a contraindication to any brow lift; the dearth of eyelid skin is often the result of a previous resection for upper eyelid ptosis, without the realization that a brow lift was indicated. As with any periocular surgery a history of “dry eye” should be elicited, for surgery has the potential to cause or exacerbate this condition.
-
Direct brow lift. Typical patient for direct brow excision (McKinney, 1991). Courtesy of Springer-Verlag. Used with permission.
-
Direct brow lift. Innervation by the supraorbital and supratrochlear nerves (Seckel, 1994). Courtesy of Quality Medical Publishing. Used with permission.
-
Direct brow lift. Ideal brow position.
-
Marking for direct brow lift.
-
Direct brow lift. Preoperative marking for eyebrow ptosis after partial facial nerve resection.
-
Direct brow lift. Excision to the level of the frontalis.
-
Direct brow lift. Beveling the incision.
-
Direct brow lift. Injury to the temporal (frontal) branch of the facial nerve in a patient referred for treatment.
-
Direct brow lift. Fixation of brow and closure.
-
Direct brow lift. Placement of deep dermal sutures.
-
Direct brow lift. Closed wound.





