Background
The forehead lift, or brow lift, is a common facial rejuvenation procedure, performed as an isolated technique or in combination with total facial rejuvenation, including facelift and blepharoplasty. [1] Clinical data and paradigm shifts have reoriented the term brow lift as a misnomer; the terms browplasty or brow reshaping focus on the overall contour rather than the absolute height of the brow. [2, 3]
A survey by Fabi et al of facial aesthetics–related priorities and concerns worldwide found that forehead lines came in third (31%) with regard to which of 25 aspects of the face respondents were highly or extremely concerned about. The most concern was garnered by under-eye bags and dark circles (36%) and crow’s feet (34%). Survey respondents consisted of more than 14,500 adults considered to be “aesthetically conscious,” including over 1300 physicians (the largest share of whom were dermatologists and plastic surgeons). [4]
Problem
Periorbital changes are often recognized as the earliest signs of aging. Common changes include upper eyelid skin folds extending beyond the upper eyelid into the temple, frown lines or glabellar transverse forehead creases, thickening or bunching of the corrugator muscles at the medial eyebrow, and descent (ptosis) of the eyebrows. See the images below.

These changes potentially are reversed with an appropriately performed brow lift or forehead lifting procedure.
In this discussion, the terms brow lift and forehead lift are used interchangeably. The actual incision used to perform a brow lift can vary from the coronal line, the prehairline, and just above the eyebrow. This topic focuses on the indications, techniques, and results of the coronal approach. For information on other brow lift procedures, see the Brow Lift section of Medscape’s Plastic Surgery journal.
Epidemiology
Frequency
Aging varies in each individual. Forehead changes are based on environmental factors (sun damage), genetic makeup, and skin type. The extent of aging can vary greatly.
Beginning in the fourth decade, early changes of brow position, influenced by gravity, become apparent. This eventually occurs in all individuals, although the degree of brow ptosis and constellation of findings such as glabellar frown lines and transverse forehead creases vary. By the fifth decade, most individuals have undesirable changes of the forehead and upper periorbital region that would benefit from rejuvenative forehead procedures.
Etiology
The etiology of the aging upper face involves loss of elasticity, soft tissue ptosis, genetic predisposition, and repetitive facial motion (eg, squinting, constant corrugation of eyebrow muscles).
Individuals with active facial animation, especially those who are exposed to sun, may exhibit more advanced signs of upper forehead aging.
Pathophysiology
Constant motion of the frontalis muscle creates the transverse rhytides of the forehead. Patients with advanced brow ptosis activate the frontalis muscles on a regular and involuntary basis to maintain elevation of their brows, thereby preventing the visual field obstruction that occurs from brow ptosis. As forehead soft tissues continue their descent over time, compensatory frontalis muscle tone creates progressively deepening lines to offset the effect on visual field obstruction.
In such cases, the well-intentioned removal of upper eyelid skin can create further brow ptosis through a relaxation in frontalis tone, which is now no longer required to maintain the visual field. The removal of upper lid skin in such cases can make later brow elevation more complicated, with poorer aesthetic results due to the limitations created by a paucity of upper lid skin. To overcome this deficiency, skin grafts or flaps from the lower lid may be considered. Remarkable aesthetic improvements can be achieved with techniques that diminish frontalis tone and weaken the centralizing and depressing muscular action while elevating the brow to an appropriate position.
Presentation
Patients may be told by family, friends, or colleagues that they appear angry, sad, or anxious when this appearance does not match their emotional state. This misinterpretation can be quite concerning for some and may result in a visit to a plastic surgeon for treatment. Elevating the brow while diminishing corrugator and procerus function can reduce forehead rhytides. This goal is accomplished through a skillfully performed brow lift.
Indications
A brow lift may be indicated in anyone who approaches the fourth decade of life and exhibits changes such as brow ptosis and excess corrugator action with glabellar creases between the eyebrows and transverse forehead wrinkling. Many of these patients are motivated to change the unacceptable appearances of anger, annoyance, or fatigue that commonly are associated with changes in the forehead.
In the female patient, elevation of the lateral eyebrow and weakening of the centralizing and depressor muscles provides a more aesthetically pleasing upper periorbita, consistent with youthful femininity.
In men, eyebrow position also may be excessively low, and elevation may be indicated; however, excessive elevation can be feminizing. Vertical glabellar frown lines may suggest anger or anxiousness and are typically undesirable. Concerns over the appearance of these unwanted lines often prompts a visit to a plastic surgeon.
Relevant Anatomy
A thorough knowledge of the layers of the scalp and forehead is paramount. The layers encountered in brow lift surgery are the skin, subcutaneous tissue, galea or aponeurosis, loose areolar tissue plane, and periosteum. Progressing inferiorly from the coronal or hairline incision, the deep and superficial layers of the temporal fascia are encountered laterally; an understanding of these layers and how they relate to the frontal branch of the facial nerve as it traverses the galea and superficial musculoaponeurotic system (SMAS) layer is critical. [5] See the image below.
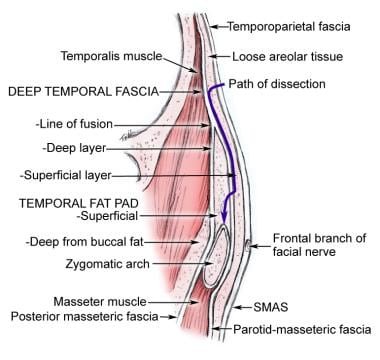 Cross-section of the temporal region showing fascial relationships to the zygomatic arch.
Cross-section of the temporal region showing fascial relationships to the zygomatic arch.
A brow lift may be performed via a subcutaneous, subgaleal, or subperiosteal layer. Most brow lifts are performed through an open technique in a subgaleal fashion, with release of soft tissue attachments at the supraorbital rim to make transmission of lift to the lateral eyebrow possible.
Anatomic understanding of the supraorbital and supratrochlear nerve branches that traverse the medial eyebrow region also is important. Supratrochlear nerves are invested within the corrugator muscle. They are visualized in dissection and removal of the corrugator muscle and must be preserved. The supraorbital nerve exits more lateral than the supratrochlear nerves and provides sensation to the hemi-forehead, extending superiorly above the hairline. Preserving these nerves minimizes sensory deficiencies.
The frontal branch of the facial nerve is carried in the forehead flap when the procedure is performed through the subgaleal or subaponeurotic dissection. Tension or traction on the forehead flap at the level of the lateral orbital rim must be gentle to avoid neurapraxia or permanent injury to the nerve.
An intimate knowledge of the insertion and origin of the corrugator muscles, procerus muscle, and frontalis muscle is essential to performing a comprehensive brow lift procedure that reverses the signs of aging.
For more information about the relevant anatomy, see Forehead Anatomy.
Contraindications
The most significant contraindication to a forehead lift is deficiency of upper eyelid skin. This often occurs when previous upper eyelid surgery has been performed, lagophthalmus has occurred, and adequate lid closure is a concern. Elevation of the brow to its proper level may be impossible if adequate upper eyelid skin is not present. This demonstrates the importance of proper diagnosis in the aging face so that excess upper eyelid skin is not removed simply because this is the "easier way out."
In most patients, a properly performed brow lift is the cornerstone of upper facial rejuvenation. Only after placing the brow in the proper position can one assess excess upper eyelid skin. This is especially true in women, in whom eyebrow position and shape is quite important in establishing the aesthetics of the periorbital region. A properly arched and elevated lateral brow is a key element to a rejuvenated female face.
A relative contraindication to a coronal forehead lift is a preexisting high anterior hairline. When excessively high, a coronal brow lift exacerbates this aesthetic problem. Further, following a coronal brow lift, performing subsequent hairline brow lifts to correct the problem is difficult without jeopardizing the vascularity to the intervening scalp segment that contains the anterior hairline. The endoscopic and prehairline brow lifts do not significantly alter hairline position and, therefore, are more appropriate choices for patients who have high anterior hairlines. However, studies suggest limited and often incomplete excursion of the lateral brow via the endoscopic approach. [3] The direct lateral brow lift has thus gained significant favor owing to its technical ease and reliability. [6]
-
Cross-section of the temporal region showing fascial relationships to the zygomatic arch.
-
Method for quantitative topographic assessment of age related brow changes and operative technique.
-
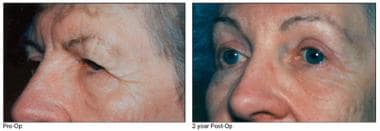
Left - Preoperative view, brow lift Right - Postoperative view at 2 years
-
Left - Preoperative view, brow lift Right - Postoperative view at 2 years
-
Left - Preoperative view, brow lift Right - Postoperative view at 2 years
-
Left - Preoperative view, brow lift Right - Postoperative view at 2 years





