Practice Essentials
Dupuytren disease (DD) is a fibrosing disorder that results in slowly progressive thickening and shorting of the palmar fascia and leads to debilitating digital contractures, particularly of the metacarpophalangeal (MCP) joints or the proximal interphalangeal (PIP) joints. This condition usually affects the fourth and fifth digits (the ring and small fingers). [1] See the images below.
 Arrow denotes the cord often present in Dupuytren contracture. Metacarpophalangeal joint and proximal interphalangeal joint contractures are also present.
Arrow denotes the cord often present in Dupuytren contracture. Metacarpophalangeal joint and proximal interphalangeal joint contractures are also present.
 Dupuytren contracture. This photo shows a patient with an inability to extend the fourth and fifth digits. The differential diagnosis includes Dupuytren contracture, which is a flexion contracture most commonly involving digits 4 and/or 5.
Dupuytren contracture. This photo shows a patient with an inability to extend the fourth and fifth digits. The differential diagnosis includes Dupuytren contracture, which is a flexion contracture most commonly involving digits 4 and/or 5.
Dupuytren contracture belongs to the group of fibromatoses that include plantar fibromatosis (Ledderhose disease), penile fibromatosis (Peyronie disease), and fibromatosis of the dorsal PIP joints (Garrod nodes or knuckle pads). [2] Although many cases appear to be idiopathic, both a genetic component and ocupational factors have been reported. [3, 4]
Dupuytren contracture is most commonly observed in persons of Northern European descent and affects 4-6% of Whites worldwide. [5, 6] The incidence increases with age; many patients are over 50 years old. [6] Many cases are bilateral (45%); in unilateral cases, the right side is more often affected. [7] The ring finger is most commonly involved, followed by the fifth digit and then the middle finger. The index finger and the thumb are typically spared.
Males are three times as likely to develop disease and are more likely to have higher disease severity. [8, 9] Male predominance may be related to expression of androgen receptors in Dupuytren fascia. [10]
Other potential risk factors include manual labor with vibration exposure, prior hand trauma, alcoholism, smoking, diabetes mellitus, hyperlipidemia, Peyronie disease, and complex regional pain syndrome. [11] Rheumatoid arthritis seems to protect against the development of Dupuytren disease.
Therapies include conservative medical and surgical modalities. Although the condition is not fatal, significant morbidity can occur if patients are untreated.
Stages of Dupuytren disease
Dupuytren disease occurs in the following three stages:
-
Proliferative phase - During this phase, myofibroblasts proliferate and a nodule develops. In early disease, some patients may report tenderness and discomfort associated with the nodules. The associated pain is thought to be due to nerve fibers embedded in the fibrous tissue or compression of local nerves. [12] On physical examination, palmar skin blanching is seen with finger extension.
-
Involutional phase - In this phase the disease, spreads along the fascia and into the fingers, resulting in the development of a cord. Myofibroblasts are the predominant cell type during this phase and align themselves along tension lines within the nodule
-
Residual phase – During the residual phase, the disease continues to spread into the fingers and the cord tightens, creating a contracture. The nodular tissue disappears, as do the myofibroblasts, and acellular tissue with thick bands of collagen remains.
Dupuytren disease is not always progressive, however. A prospective study in 247 Dutch participants with primary Dupuytren disease with follow-up at intervals of 3 to 6 months found that in up to 75% of patients, the disease stabilizes or even regresses. [13]
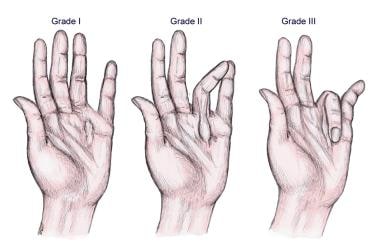
Grades of severity
The grading system for Dupuytren disease severity is as follows (see the images below) [14] :
-
Grade 1 - Thickened nodule and band in the palmar aponeurosis; may have associated skin abnormalities
-
Grade 2 - Development of pretendinous and digital cords with limitation of finger extension
-
Grade 3 - Presence of flexion contracture
See the images below.
Arrow denotes the cord often present in Dupuytren contracture. Metacarpophalangeal joint and proximal interphalangeal joint contractures are also present.
 Arrow denotes the typical cords of Dupuytren contracture. These cords are usually painless. Note the metacarpophalangeal joint contracture.
Arrow denotes the typical cords of Dupuytren contracture. These cords are usually painless. Note the metacarpophalangeal joint contracture.
 Dupuytren contracture. This photo demonstrates the presence of a nodule as well as skin blanching with extension of the affected digits.
Dupuytren contracture. This photo demonstrates the presence of a nodule as well as skin blanching with extension of the affected digits.
Treatment
A variety of non-surgical and surgical options are available for management of Dupuytren disease. The choice largely depends on the severity of disease, degree of deformity, limitations in function, and provider preference. Collagenase injection followed by rupture of the pathologic cord through passive extension has become a first-line treatment. [15] Surgical procedures are reserved for patients with contractures > 30-40º or with significant disability. [16] In advanced cases a variety of techniques may be used to prevent recurrence (eg, skin grafting, external fixator application, radiation). [17]
Background
The eponymic term for this disorder honors the French surgeon Guillaume Dupuytren, who described the contracture in 1833. Several earlier descriptions of the condition exist in the medical literature, however. [2]
Anatomy
In the normal hand, the palmar aponeurosis runs longitudinally from the wrist, crosses over the superficial transverse palmar ligament, and splits into pretendinous bands to each digit. See the image below.
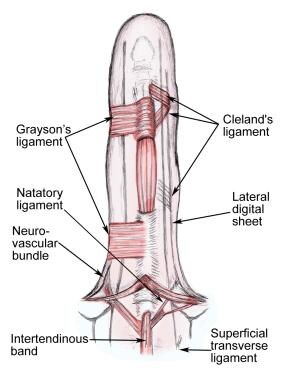
In the distal palm and fingers, the following superficial fascial components are typically involved in Dupuytren disease:
-
Pretendinous band
-
Spiral band
-
Lateral digital sheet
-
Grayson ligament
-
Natatory ligament
The extension of a palmar fascial band to the index finger frequently ends in the skin on the radial side of the hand. The band to the thumb is inconsistent. The insertion of the pretendinous bands to the skin distal to the distal palmar crease is by means of a bifurcate insertion into the side of the finger dorsal to the neurovascular bundle. A natatory ligament runs transversely across each web space distal to the MCP joint, giving fibers that blend with each lateral digital sheet and to the superficial aspect of the flexor tendon sheath. The superficial transverse ligament lies deep to the pretendinous bands, proximal to the MCP joints and the natatory ligament. In the fingers, the Cleland ligament, Landsmeer ligaments (oblique retinacular ligaments), and other deeper fascial layers are usually spared in Dupuytren disease. [18, 19, 20]
According to Luck, normal longitudinal components of the superficial palmar aponeurosis are referred to as bands; diseased tissue is referred to as cords. [21] Cardinal features of Dupuytren disease are the nodule, the cord, and the digital flexion contracture. The bands and cords are characterized as follows:
-
The pretendinous cord is formed from pretendinous bands.
-
The spiral cord is made up of the pretendinous band, spiral band, lateral digital sheet, and Grayson ligament; this often occurs in the ring and small fingers and winds around the neurovascular bundle.
-
The lateral cord is formed from the lateral digital band and is rarely observed, except on the ulnar aspect of the small finger.
-
The central cord has no defined fascial precursor; it is the most common cause of proximal PIP contracture.
-
The natatory cord contributes to web space contractures and passes superficial to neurovascular bundles.
See the images below.
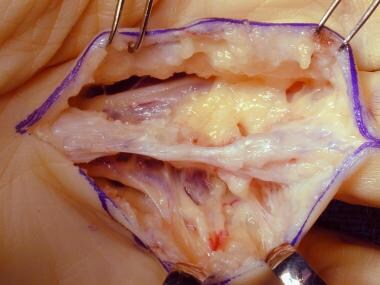
 Visible cord characteristic of Dupuytren disease with planned markings for surgical release.
Visible cord characteristic of Dupuytren disease with planned markings for surgical release.
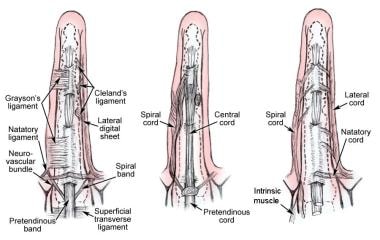 Parts of the palmar and digital fascia that become diseased in Dupuytren disease (left). Diseased fascia that is associated with the pretendinous cord (center). Diseased fascia that is not associated with the pretendinous cord (right).
Parts of the palmar and digital fascia that become diseased in Dupuytren disease (left). Diseased fascia that is associated with the pretendinous cord (center). Diseased fascia that is not associated with the pretendinous cord (right).
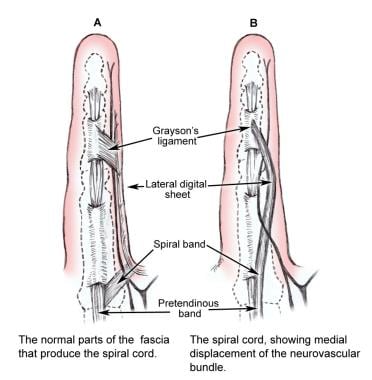 Dupuytren contracture. The drawing on the left shows the normal parts of the fascia that produce the spiral cord. The drawing on the right shows the spiral cord and medial displacement of the neurovascular bundle in Dupuytren disease.
Dupuytren contracture. The drawing on the left shows the normal parts of the fascia that produce the spiral cord. The drawing on the right shows the spiral cord and medial displacement of the neurovascular bundle in Dupuytren disease.
Spiral and lateral cords displace the neurovascular bundle toward the digital midline, while a central cord may encase the neurovascular bundle and usually is directed toward one side of the finger. The central, lateral, and spiral cords terminate on the tendon sheath of the adjacent middle phalanx. One or more may be found in any individual patient, but they seldom occur on both sides of the same finger. McFarlane describes displacement of the neurovascular bundle superficially and toward the digital midline by a spiral cord, which makes it more vulnerable to injury during surgery. [20] With increasing degrees of flexion contracture, nerve compression and vascular embarrassment may also occur.
In the thumb, 3 fascial structures may be involved: the natatory ligament, the pretendinous band, and the superficial transverse ligament of the palm. Knuckle pads may develop with fibrosis in the dorsal subcutaneous wrinkle ligaments (of McGrouther) dorsally at the PIP joints. These often indicate progressive disease.
Pathogenesis/Etiology
Although the underlying etiology for the development of Dupuytren disease is uncertain, the basic pathophysiology involves fibroblast proliferation, and collagen deposition leading to contractures of the palmar fascia. Investigators have proposed several hypotheses for the pathogenesis of Dupuytren disease. Al-Qattan hypothesizes that an individual with a genetic predisposition to develop Dupuytren disease experiences a second inciting event (ie, smoking, diabetes, trauma, alcoholism), resulting in microvascular ischemia. [10] The localized ischemia causes two events to take place in the palmar fascia: (1) the conversion of adenosine triphosphate to hypoxanthine and (2) the conversion of xanthine dehydrogenase to xanthine oxidase.
Xanthine oxidase acts as a catalyst for the oxidation of hypoxanthine to xanthine and uric acid; this conversion results in the production of free radicals. Free radicals result in fibroblast proliferation and the production of numerous cytokines. Interleukin 1 (IL-1) is the most abundant cytokine in Dupuytren disease and, via its receptor, upregulates the production of transforming growth factor beta (TGF-beta), fibroblast growth factor, epidermal-derived growth factor, and platelet-derived growth factor. [22, 23] This milieu of cytokines and growth factors results in the proliferation of fibroblasts and their differentiation into myofibroblasts (the primary cell type in Dupuytren disease). [24]
Increased levels of nerve growth factor are present, which induce fibroblast transformation to myofibroblasts, especially during stages II-III. The splicing of fibronectin affects collagen binding. Platelet activation produces lysophosphatidic acid (LPA). LPA is a signaling molecule for cell proliferation and myofibroblast contraction. After binding to its receptor on myofibroblasts, LPA leads to a decrease in cyclic adenosine monophosphate and an increase in intracellular calcium levels. These events mediate smooth muscle contraction of the myofibrils within the myofibroblast. Normal palmar fascia is primarily composed of type I collagen; Dupuytren disease is associated with an increase in type III collagen.
The ratio of type III collagen to type I collagen increases, the reverse of the normal pattern, in the palmar fascia. [14] Excess type III collagen production occurs from an increased density of fibroblasts secondary to enhanced stimulation and diminished apoptosis, as well as an imbalance between the collagenases and their endogenous inhibitors. Dupuytren fascia exhibits an increased ratio of tissue inhibitors of metalloproteinases (TIMP) to matrix metalloproteinases (MMP). [25, 26, 27]
The myofibroblasts are indirectly connected to collagen, and the contractile force is transmitted from the intracellular actin microfilaments to the collagen bundles. Ultimately, the end result is contracture from excess deposition of type III collagen and the formation of cross-links between myofibroblasts and collagen. Another hypothesis by Vi et al suggests an up regulation of the gene transcript POSTN mRNA that encodes the protein periostin. Periostin is secreted by diseased cord myofibroblasts into the extracellular matrix. It promotes the transition of palmar fascia fibroblasts into a myofibroblast phenotype, thereby enhancing disease progression. [28]
Additionally, periostin is prevalent during the early stages of bone fracture repair and vascular injury. Hueston advanced the extrinsic theory, suggesting that Dupuytren nodules arise de novo and progress to cords. [29] Vasomotor disturbance and neurovascular mediation by the skin are possible contributors to the development of Dupuytren disease.
In contrast, McFarlane postulated the intrinsic theory, that the cords of more advanced Dupuytren disease are derived from normal fascia. [20] A combination of these ideas forms the synthesis theory, which states that the nodules and pretendinous cords represent different forms of the disease. [30]
Genetic factors
Though the cause of Dupuytren contracture remains unknown, genetic factors are thought to play a role. [31] One study derived a sibling recurrence-risk ratio of 2.9 (range, 2.6-3.3). [32]
Furthermore, DNA microarray analysis has demonstrated that the gene MafB is up-regulated in Dupuytren cord tissue. MafB is involved in tissue development and cellular differentiation. [33, 32] Further support for a genetic link was provided by Al-Qattan, who described a maternally transmitted inheritance within the mitochondrial genome in 90% of patients. The defective mitochondria generate high levels of free radicals and defective apoptosis and are therefore directly related to disease pathogenesis. [10]
Another study of 20 patients with apparent maternal inheritance identified a polymorphism in the mitochondrial 16s rRNA region present in 90% of their DNA. [34] Other studies suggest an autosomal dominant pattern of inheritance with variable penetrance. [35] One such study analyzed 5 generations of a Swedish family and mapped the affected gene (not yet identified) to 16q. [36] Some authors suggest an error in growth and regulation of the fibroblast resulting from chromosomal abnormalities, similar to those seen in cells undergoing neoplastic changes. Trisomy 7 and 8 have been identified in the fibroblasts excised from some patients. [37] Nodules may display features of a benign neoplasm. [38]
A genomewide association study of 960 persons with Dupuytren disease and 3117 controls—all from the Netherlands and of European descent—identified 11 single-nucleotide polymorphisms (SNPs) from nine different loci involved in genetic susceptibility to Dupuytren disease. Six of the nine loci harbor genes encoding proteins in the Wnt-signaling pathway, which is known to regulate the proliferation and differentiation of fibroblasts in fibromatosis. [39]
Others believe that Dupuytren contracture has a multifactorial inheritance, similar to diabetes or hypertension.
Additional risk factors
Whether certain conditions represent independent risk factors for the development of Dupuytren contracture is unclear. A large, retrospective study by Loos and colleagues on 2919 hands on which surgery had been performed revealed no statistically significant evidence that the occurrence of Dupuytren contracture could be correlated with the presence of diabetes, with alcoholism, or with smoking. [38]
Another report, however, found different results, noting an association between Dupuytren contracture and several conditions (eg, alcoholism, diabetes, epilepsy, pulmonary disease), as well as a link with smoking. [40] Nonetheless, even if such associations exist, no clear causal relationship has been established in the literature.
HLA-DRB1*15 and HLA-DR3 have been identified in numerous patients, suggesting an immunologic influence. Each confers about a 2-3 times relative risk for the development of Dupuytren disease. [41, 42] Most likely, an inciting disease or event in a genetically predisposed individual causes a cascade of events that may include processes that promote the formation of growth factors and free radicals that ultimately leads to abnormal fibroproliferation and the appearance of the characteristic Garrod nodule. Even when homeostasis is ultimately achieved and fibroblastic growth lessens, the pathologic nodule and cord remain.
Many hand surgeons believe that trauma to the hand or the distal part of the forearm, such as falling on an outstretched hand, may precipitate the onset. [43] (A positive family history may play a role in occupational and traumatic cases of Dupuytren disease.) However, numerous population-based studies have failed to conclusively link Dupuytren disease to trauma, [44] although case reports have suggested a possible association. [45] Reports by Lucas et al found increased Dupuytren disease in a group of French male civil servants with occupational exposure to vibration and manual work. [46]
Case reports of Dupuytren disease occurring after surgical injury to the hand have been identified, with the authors suggesting that injury can trigger the onset of Dupuytren disease. [47] A history of manual labor with vibration exposure or recurrent trauma has been found to result in a 5-fold increase in the incidence of Dupuytren disease. [48, 49, 50] Liss performed a systemic review of the literature regarding occupation and Dupuytren disease. Although he failed to identify a link between trauma and development of disease, he did find an association between occupational exposure to vibration and Dupuytren disease. [44]
Notably, the exposure in one study was severe enough to cause persistent symptomatic circulatory disturbance ("vibration white finger") [48] ; in another, the exposure was associated with other soft tissue "wasting" and peripheral nerve damage. In a review of 46 available studies, Melhom and Ackerman concluded evidence suggests an association between Dupuytren disease and vibration but not with highly repetitive or forceful work. [51]
Diabetes mellitus has been identified as a risk factor. [52] Dupuytren disease in patients with diabetes ranges from 1.6-32%, the prevalence of diabetes in patients with Dupuytren disease is 5%. [8] The use of insulin and oral hypoglycemics are strongly associated with Dupuytren disease. The disease seems to occur at a younger age and tends to be more severe in those with type 1 diabetes. [53]
Patients with diabetes mellitus and Dupuytren disease have a 4-fold increased risk of developing microalbuminuria than do persons with diabetes alone. [54] A higher incidence of retinopathy was identified in diabetics with Dupuytren contracture, likely attributable to microangiopathic changes. Alcoholic liver disease Individuals with alcohol-related liver disease have an increased prevalence of Dupuytren contracture (approximately 20%) compared with control populations. Patients with liver disease from other causes do not appear to be at increased risk. The reason for this is unknown, and some studies have disputed the association. [55]
A 3-fold increased risk for Dupuytren contracture is seen in individuals who smoke, even when studies control for alcohol use, perhaps due to microvascular impairment. [40] Autoantibodies to connective tissue Significant associations have been found with HLA-DRB1*15, HLA-DR3 and autoantibodies to collagen types I-IV have been reported. [56]
Two studies have shown increased sensitivity to androgens in the palmar fascia. [57, 58] This may account for the male predominance of the disease.
Although implicated in previous studies, little conclusive evidence has been reported to link epilepsy and antiepileptic medications to the development of Dupuytren contracture. Phenobarbitone, in particular, results in increased LPA levels. Although the incidence of Dupuytren disease is 2-3 times higher in individuals with epilepsy, opinions about the cause differ. One group of investigators concluded that electroencephalogram (EEG) abnormalities were more common in patients with Dupuytren disease than in persons with other clinical conditions.
Another study showed a correlation between increased barbiturate medication and a higher occurrence of Dupuytren disease, whereas other studies implicated a genetic link between the two diseases. [59]
Results are conflicting as to whether the human immunodeficiency virus (HIV) is implicated in some cases of Dupuytren disease. [60] Bower et al demonstrated an increased incidence in patients with both Dupuytren contracture and HIV infection, whereas a study by French et al showed no statistically significant difference in these patients compared with the general population. [61]
Epidemiology
Frequency
Dupuytren disease occurs most often in persons of northern European ancestry. [62] Dupuytren disease is common in the United States with a prevalence of 4%, reflecting immigration from Northern Europe. [14] In Northern Europe the prevalence ranges from 4-39%. In Norwegian populations, 30% of males over the age of 60 years are affected. The incidence of Dupuytren disease for the British population in 2004 was calculated at 34.4 per 100,000 for men aged 40-84 years. [14] Australia has a reported prevalence of 28%; Spain's reported prevalence is 19% prevalence in in men older than 60 years. [7] Sporadic cases are reported in Africa and Asia. [14]
Race
Racial variation in Dupuytren disease is as follows:
-
Dupuytren disease is most often found in Whites of Northern European descent.
-
The disease prevalence in Asians is 3% and usually involves the palm rather than the digits. Therefore, it is less likely to be clinically significant, and the incidence may be underreported.
-
Dupuytren disease has been reported in East Africa, Zimbabwe, and Tanzania. [11]
-
Dupuytren disease is uncommon among Indians (< 1%), Native Americans, and patients of Hispanic descent. [11]
Sex and age
Approximately 80% of affected individuals are male; this is consistent throughout all countries and races. The disease onset in males tends to occur in the fifth to sixth decade. Men tend to present a decade earlier than females. The disease course tends to be more rapid and severe in males and increases in incidence with advancing age. [54]
Dupuytren disease is rare in children younger than 10 years. Only eight histologically proven cases have been reported. [63]
Prognosis
The effects of morbidity in Dupuytren contracture are generally limited to lifestyle changes. MCP and PIP joint contractures may interfere with activities of daily living and the nodules can be painful. Occasionally, Dupuytren contracture is associated with plantar fascial thickening (Ledderhose disease), involvement of the penis (Peyronie disease), or involvement of the knuckle pads (Garrod nodes). These associations tend to reflect more aggressive disease. [64] No mortality occurs from Dupuytren contracture.
A population-based retrospective review of 593,606 patients were diagnosed with trigger finger found 15,416 (2.6%) developed trigger finger after a diagnosis of Dupuytren disease. Another 2603 (0.4%) developed trigger finger after treatment for Duputren disease. Patients treated surgically with fasciectomy or fasciotomy were more likely to develop trigger finger than those who received collagenase clostridium histolyticum (CCH) injection. [65]
Patient Education
Patients must have realistic expectations that surgery can relieve some disability but that it cannot cure Dupuytren disease. Discuss all potential complications of the procedure, including complex regional pain syndrome. In addition, intensive rehabilitation with an occupational therapist is necessary postoperatively for an optimal outcome.
-
Arrow denotes the cord often present in Dupuytren contracture. Metacarpophalangeal joint and proximal interphalangeal joint contractures are also present.
-
Arrow denotes the typical cords of Dupuytren contracture. These cords are usually painless. Note the metacarpophalangeal joint contracture.
-
Dupuytren contracture. This photo demonstrates the presence of a nodule as well as skin blanching with extension of the affected digits.
-
Ultrasound of the palm in Dupuytren disease of the fourth digit; the Dupuytren nodule and thickening of the palmar fascia with puckering of the skin is noted. Green arrow: Flexor tendon; Red arrow: Dupuytren nodule; Blue arrow: Thickened palmar fascia; Yellow arrow: Puckering of the skin.
-
Dupuytren contracture. This photo shows a patient with an inability to extend the fourth and fifth digits. The differential diagnosis includes Dupuytren contracture, which is a flexion contracture most commonly involving digits 4 and/or 5.
-
Visible cord characteristic of Dupuytren disease with planned markings for surgical release.
-
Dupuytren contracture. Dissection of a diseased cord.
-
Dupuytren contracture. Normal anatomy of digital ligaments.
-
Three clinical grades of Dupuytren disease.
-
Parts of the palmar and digital fascia that become diseased in Dupuytren disease (left). Diseased fascia that is associated with the pretendinous cord (center). Diseased fascia that is not associated with the pretendinous cord (right).
-
Dupuytren contracture. The drawing on the left shows the normal parts of the fascia that produce the spiral cord. The drawing on the right shows the spiral cord and medial displacement of the neurovascular bundle in Dupuytren disease.




