Practice Essentials
Acquired ear deformities are typically the result of trauma, skin lesion excisions, and hematomas or infections. The critical reconstruction issues for each of these 3 etiologies are different.
The success of ear reconstruction after trauma depends on two main factors. The first of these is vascular patency. The survival of a reconstructed auricle depends on sufficient arterial inflow to nourish the healing graft. Also, venous congestion caused after partial or total amputation can result in cartilage loss. The second factor concerns the availability of soft tissue cover over reimplanted or harvested cartilage framework. Lack of soft tissue cover following a traumatic injury can limit the options available for repair or can require more complex flap coverage.
Obtaining a balance between size and shape is the most important factor for reconstructions after skin lesion excision. To make the ear appear normal, the surgeon must often sacrifice the size of the underlying cartilage to preserve a normal shape and avoid distortion. Because both ears are not typically seen at the same time, the preservation of anatomic landmarks is more important than maintaining symmetry of size.
Ear reconstruction after infections or hematomas depends on the amount of remaining cartilage support. More extensive cartilage framework involvement in infections or hematomas requires more debridement. Extensive cartilage loss may result in a total ear reconstruction similar to that needed for a congenital ear deformity.
This discussion presents basic plastic surgery principles and their application to acquired ear deformities. The subject of traumatic lesions to the ear is followed by techniques for repair following controlled extirpations of skin lesions. Many of the techniques described for reconstruction of skin lesion excision can be used in traumatic lesion reconstructions and vice versa.
Management
Surgery for ear reconstruction and salvage can be accomplished with the following
-
Skin grafts
-
Cutaneous flaps - Thin-tubed flaps, banner flaps, mastoid flaps
-
Chondrocutaneous flaps - Antia-Buch chondrocutaneous advancement flap, chondrocutaneous conchal flap, island chondrocutaneous postauricular flap
Specific reconstruction and salvage techniques include the following:
-
Pocket principle
-
Microvascular replantation
History of the Procedure
See the list below:
-
Ear reconstruction has a long and varied history. An 8th-century Indian text, the Susrata, contains one of the first recorded descriptions of ear reconstruction (the use of a cheek flap to repair an earlobe defect.) A report from 1551 contains the first the description of a total ear replantation. [1] By 1920, Gillies was using autologous cartilage for total ear reconstructions. This evolution stemmed from the need to cope with the results of congenital ear deformities. In 1959, Tanzer ushered in the modern era in ear reconstruction with the successful use of autologous costal cartilage grafts. [2, 3] Brent advanced the standards of ear reconstruction with autogenous materials and was the first to report the successful use of tissue expansion in reconstruction of the ear. [4] Many of the innovative techniques used for total reconstruction of congenital ear defects can be applied to acquired defects.
Epidemiology
Frequency
Approximately 800,000 people develop skin cancer in the United States every year. Of these, 90% are due to lesions in the head and neck region, 12% of which involve lesions on the ear and periauricular area. Fifty to sixty percent of all skin lesions of the external ear are squamous cell carcinomas, 30-40% are basal cell carcinomas, and only 2-6% are melanomas. The helix is involved in 45-55% of these lesions. Approximately one-third of cutaneous carcinomas of the ear extend directly in the underlying cartilage and require through-and-through excision. [5]
A 10-year, retrospective study from Finland, by Korhonen et al, found the sex-based difference in cutaneous squamous cell carcinoma location to be greatest for the ear, with men accounting for 93% of these cases. [6]
The external auricle has a high potential for injury due to its exposed and unprotected position alongside the head. A retrospective study by Bardsley and Mercer looking at hospital records in auricular injury cases revealed that human bites constitute the most common cause of injury (42%). [7] This was followed by falls (20%), automobile accidents (16%), and dog bites (14%). The most common injury observed was incomplete amputation of the ear, usually helical rim tissue loss. Untreated open auricular injuries invariably result in infection, ensuing deformities, and further tissue loss. For more information on treating all kinds of trauma, visit Medscape's Trauma Resource Center.
Etiology
Acquired defects and deformities of the auricle have various causes. Common etiologies are listed below. [8]
Abrasions
Abraded areas must be cleaned and thoroughly irrigated. Debris must be removed fully and aggressively, often with sharp debridement. The involved area should be covered with topical antibiotic impregnated gauze for 24 hours. Thereafter, these injuries need to be treated as open wounds, taking care to keep the area moist with topical antibiotic ointment. Dilute 3% hydrogen peroxide can be used to remove crusting from dried blood and other secretions. Secondary epithelialization should be complete in 7-10 days. Antibiotic coverage for contaminated wounds should include pseudomonal coverage.
Aplasia
Congenital deformities of the auricle require auricular reconstruction in staged procedures. Total auricular reconstruction is beyond the scope of this article.
Avulsion and amputation injuries
Auricle avulsion or amputations may present with the complete involved segment or a portion thereof available for reconstruction. Isolated traumatic ear amputation is an uncommon event and frequently occurs in conjunction with major systemic or head and neck trauma. [9]
Blunt trauma
Injuries to the auricle from blows to the head commonly result in hematoma and seroma formation on the anterior surface of the ear between the cartilage and the perichondrium. If not corrected, fibroneocartilage forms in this area and a permanent deformity of the ear known as "cauliflower ear," shown below, may result. Acute treatment involves drainage of the effusion via needle aspiration or incision followed by application of a pressure dressing.

If the effusion recurs or if the injury is several days out and not drained initially, incision and debridement of the involved perichondrium and the newly formed fibroneocartilage may be necessary. A bolster dressing, topical antibiotic impregnated gauze on both sides of the auricle secured with through-and through sutures, can be used to maintain pressure on the involved area.

Burns
First, second, and third degree burns can result in a range of injuries from a simple denuding of the skin to a total loss of the ear. These injuries carry the risk of infection due to staphylococcal or pseudomonal contamination. Careful debridement is essential to prevent or limit these infections. Causative pathogens are of mixed flora; Pseudomonas aeruginosa is present in 95% of incidents. The use of prophylactic mafenide acetate (Sulfamylon) cream has decreased the incidence of chondritis from 29% of auricular burn cases to 19% of cases. Once diagnosed, suppurative chondritis can be treated with the local instillation of gentamicin, neomycin, and polymyxin antibiotics 2-5 times per day.
Composite defects
Composite defects are injuries that involve both skin and cartilage and in which a portion of the auricle is missing.
Frostbite
Temperatures of -19°F or lower usually cause injury. Frostbite is usually superficial and results in erythema and edema of the skin without (first degree) or with bullae (second degree). Deep wounds of the third and fourth degree frostbite result in necrosis of the skin without loss of the auricle and lead to complete necrosis, gangrene, and tissue loss.
Lacerations (simple vs complex)
Simple lacerations are linear defects in the skin of the auricle with no missing tissue. They usually involve skin with or without subcutaneous tissue. The cartilage is not involved; however, exposed cartilage may be encountered. This type of injury can be closed in a single layer with or without a bolster dressing.
Complex lacerations are also linear defects which involve cartilage. These injuries do not have missing skin or cartilage in the defect. Generally, multiple-layered closures including perichondrium are required with a bolster dressing. Bolster dressings are important to avoid hematoma formation. For a detailed description of repair, see eMedicine Clinical Procedures article Complex Laceration, Ear.

Superficial defects (perichondrium present vs perichondrium absent)
Superficial defects are injuries in which an area of skin is avulsed and missing from the underlying cartilage. These injuries may have perichondrium present or absent from the cartilage. The presence of perichondrium must be determined, as it is highly vascular and essential for cartilage survival. This allows determinations of the type of reconstruction allowable. Nonstructural defects of the conchal bowl or those between the helix and antihelix do not need reconstruction with cartilage, unlike the helical rim.
Relevant Anatomy
The auricle is typically oriented at an anteroposterior rotational angle of 15-20°. The distance from the top of the helical crus to the lateral canthus of the eye is about 6 cm. The average height of the auricle from the top of the helix to the bottom of the lobule is about 6 cm. The normal protrusion off of the skull is 30°.
Landmarks of the auricle are identified by folds and curves in the cartilage and skin (see the image below). The anterior limit of the auricle is the tragus, a domed-shaped cartilaginous prominence oriented in a vertical place lateral to the external auditory meatus. The helix is the most prominent superior turn of the auricle and terminates anteriorly just superior to the tragus at the helical crus. Just beneath the helix is the antihelix, a fold that divides anteriorly and superiorly to form the fossa triangularis. Inferiorly, the anithelix ends as a prominence forming the antitragus. Medial to the antihelix and tragus is the cavum conchae, which is continuous with the cartilaginous portion of the external auditory canal. Hanging from the cartilaginous auricle is loose skin called the lobule.
The external ear contains a single piece of elastic cartilage with closely adherent perichondrium. The upper two thirds of the ear contain cartilage; the lower third (lobule) is absent of cartilage. The cartilage has no direct blood supply, as nutrients are supplied and absorbed directly from its overlying perichondrium. The skin of the auricle adheres tightly to the underlying cartilage and contains little subcutaneous tissue. The posterior/medial ear has more subcutaneous tissue, has a rich blood supply, and is more loosely tethered to the framework.
Three extrinsic muscles connect the auricle to the scalp: the anterior, superior, and posterior auricular muscles. The anterior ligament extends from the tragus to the root of the zygomatic process of the temporal bone. The posterior ligament passes from the posterior surface of the concha to the lateral surface of the mastoid process. The auricle is attached to the temporal bone by its fibrocartilaginous tissue.
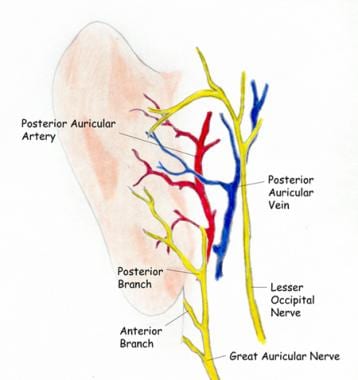
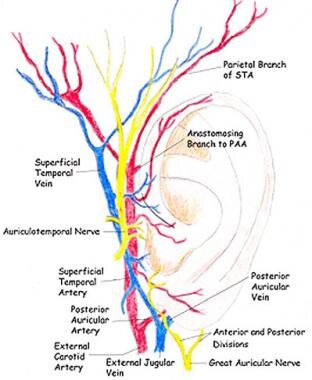
The rich auricular blood supply consists of interconnections between the posterior auricular artery (PAA) and the superficial temporal artery (STA) (see the image above). These provide extraordinary vascularization, allowing the auricle to undergo significant trauma, either surgically or accidentally, without losing its viability. The PAA supplies most of the blood to the anterior ear. It arises from the STA just below the level of the lobule. The PAA passes cephalad in the postauricular sulcus, giving branches to the medial surface of the ear. It terminates by joining a posterior branch of the STA, completing a vascular ring around the base of the ear. The STA gives off an auricular branch just anterior to the tragus. By itself, it provides a lesser contribution to the auricle. [10]
The depth of this vascular ring can vary from just a few millimeters beneath the skin to as deep as 1 cm. It supplies an area of 6 cm by 11 cm that extends from the tragus to 5 cm posterior to the external auditory canal and 6 cm inferior to the mastoid. Supply to the conchal area is derived from perforators consistently found piercing the conchal floor and originating from the PAA. Also, a rich anastomotic network exists between the PAA and the occipital artery.
A cadaver study by Gómez Díaz and Cruz Sánchez designated the area of retroauricular tissue that can safely be used in ear reconstruction, based on the tissue dimensions supplied by the PAA, finding that the artery feeds an area of retroauricular skin and fascia equivalent to 60.44 cm2. [11]
The auricle also has a rich nerve supply, which is made up of multiple cranial nerves as well as branches of the cervical plexus. The greater auricular nerve supplies most of the auricle, from the posterior/medial aspect to the anterior/lateral lobule, helix, and antihelix. It extends superiorly, where it shares innervation with the auriculotemporal nerve. The auriculotemporal nerve is a branch of the mandibular division of the trigeminal nerve (CN V3), which supplies the tragus, helical crus, and skin superior to the auricle. The lesser occipital nerve supplies skin posterior to the auricle. Cranial nerves (CN) VII and X supply most of the innervation to the cavum conchae and posterior external auditory canal arising from the middle ear. These are important to address when trying to obtain a complete nerve block when repairing the auricle.
For more information about the relevant anatomy, see Ear Anatomy.
-
Anatomy of the posterior (medial) surface of the ear.
-
Anatomy anterior (lateral) surface of the ear.
-
Cauliflower ear.
-
Drainage of effusion between cartilage and perichondrium.
-
Ear laceration.
-
Primary repair of ear laceration.
-
Different patterns of star excisions.
-
Defect ready for skin graft cover.
-
Repair with full-thickness skin graft.
-
Thin tubed flap.
-
Banner flap.
-
Tunnel procedure.
-
Antia-Buch reconstruction (1).
-
Antia-Buch reconstruction (2).
-
Antia-Buch reconstruction (3).
-
Antia-Buch reconstruction (4).
-
Chondrocutaneous conchal flap.
-
Pardue cleft earlobe reconstruction.
-
Auriculomastoid flap with a mastoid extension.
-
Retroauricular and helix/antihelix surface flaps for lobe reconstruction.





