Background
Breast reconstruction entered the modern era with the introduction of the transverse rectus abdominis myocutaneous (TRAM) flap in 1982 by Hartrampf, Scheflan, and Black. This ingenious procedure reliably transfers autogenous tissue from the abdomen for breast reconstruction and has the added benefit of abdominal rejuvenation. See the image below.
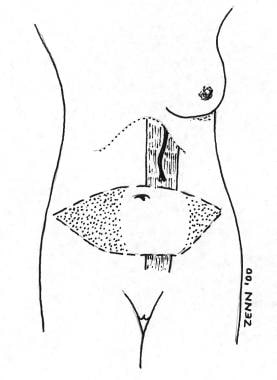 Blood supply to the unipedicled transverse rectus abdominis myocutaneous (TRAM) flap. Note the superior epigastric supply and the shaded area of the TRAM flap to be discarded.
Blood supply to the unipedicled transverse rectus abdominis myocutaneous (TRAM) flap. Note the superior epigastric supply and the shaded area of the TRAM flap to be discarded.
This procedure now constitutes 25-50% of breast reconstructions performed in the United States, and the TRAM flap has proven the autogenous tissue of choice for breast reconstruction.
The main advantage of the procedure lies in the consistency of the reconstructed breast; it is similar to the natural breast in softness and in the way the tissue drapes on the chest. Because the tissue is part of the patient's body, it does not incite foreign body reaction or capsular contractures, which have plagued implant reconstructions. Furthermore, since scars fade and tissues soften, the reconstruction only improves over time, which is not true of implant reconstructions. When performed properly in the properly selected patient, the TRAM flap procedure produces a breast reconstruction superior to any other technique. [1]
Indications
Transverse rectus abdominis myocutaneous (TRAM) flap reconstruction may be considered in any patient who is undergoing mastectomy as either an immediate procedure (at the time of mastectomy) or as a delayed procedure (sometime after mastectomy). If chest wall radiation has been or will be part of the patient's therapy, reconstruction is delayed. [2] The patient must be psychologically motivated and have adequate tissues in the abdominal area to be considered for a TRAM flap. Although implant reconstruction and tissue reconstruction may be considered for any patient, some relative indications favor the TRAM flap procedure.
-
Radical mastectomy defect with large tissue requirement
-
History of radiation to the chest wall
-
Large opposite breast (difficult to match with an implant)
-
Small opposite breast (difficult to match with an implant)
-
Previous failure of implant reconstruction
-
Excess lower abdominal tissue and patient desires abdominoplasty
Relevant Anatomy
The flap skin and fat of a single pedicle transverse rectus abdominis myocutaneous (TRAM) flap reconstruction survive on perforators through the rectus abdominis muscle. Although this muscle has a dual blood supply, the superior epigastric artery and the inferior epigastric artery, this operation relies only on the superior epigastric arterial system. Because of the distant nature of this blood supply, only tissues directly over or immediately adjacent to the muscle have adequate vascularity. If more tissues are needed, consider other procedures (midabdominal TRAM, delay procedure, double pedicle TRAM, super-charged TRAM, free TRAM flap, deep inferior epigastric perforator [DIEP] flap).
Contraindications
The transverse rectus abdominis myocutaneous (TRAM) flap operation is major surgery and should not be undertaken lightly by the patient or surgeon. Over fifteen years of experience with these procedures enables the author to identify certain characteristics that place patients at higher risk for complications.
-
Cardiac disease (ie, myocardial infarction, angina, congestive heart failure)
-
Pulmonary disease (ie, emphysema, chronic obstructive pulmonary disease)
-
History of pulmonary embolus or deep venous thrombosis
-
Collagen-vascular disease, lupus, scleroderma, polyarteritis (small vessel disease)
-
Unstable psychiatric disease
-
Obesity (>25% ideal body weight)
-
Older patient (physiologic age older than 70 y)
-
Cigarette smoking; unwilling to quit
-
Previous abdominal surgery that has interrupted blood supply to the TRAM flap
Because of the magnitude of the procedure and the degree of stress on the lungs and heart, this operation may unmask baseline cardiopulmonary disease and result in a complicated course for the patient. In addition, anything that causes small vessel disease, such as the medical conditions listed above, diabetes, or cigarette smoking, may cause complications in the transferred tissue and in the abdominal donor site. Any of the above characteristics contraindicate a TRAM flap, thus the surgeon should seek another method of reconstruction.
Patients who wish to have more children should be advised to consider another method of reconstruction, although this is not an absolute contraindication. Many reports exist of patients who have undergone TRAM experiencing full-term natural childbirth; the concern mostly centers on the diminished compliance of the abdominal wall, especially when synthetic mesh was used. Patients who desire no or little muscle to be removed with the TRAM flap should consider a free TRAM flap, deep inferior epigastric perforator (DIEP) flap, or superficial inferior epigastric artery (SIEA) flap. [3]
-
Blood supply to the unipedicled transverse rectus abdominis myocutaneous (TRAM) flap. Note the superior epigastric supply and the shaded area of the TRAM flap to be discarded.
-
Patient 1: The small-breasted patient did not want contralateral augmentation, and it would be difficult to match her breasts with an implant alone.
-
Patient 1: Postoperative view after unipedicled transverse rectus abdominis myocutaneous flap reconstruction. This small breast with ptosis would be impossible to achieve with an implant.
-
Patient 2: A full C cup breast and an ample abdomen for an unipedicled transverse rectus abdominis myocutaneous reconstruction
-
Patient 2: Postoperatively after unipedicled transverse rectus abdominis myocutaneous and nipple reconstruction. Note the improvement in the patient's abdominal appearance, a benefit of this type of reconstruction. She has been encouraged to return for re-application of the removed portion of her tattoo.
-
Patient 3: The patient's right lateral scar during initial biopsy precludes a true skin-sparing approach. With ample abdominal tissue, she is an excellent candidate for unipedicled transverse rectus abdominis myocutaneous reconstruction.
-
Patient 3: Postoperative view after unipedicled transverse rectus abdominis myocutaneous flap reconstruction. Note the abdominal skin replacing the removed skin to maintain breast shape. The patient does not desire nipple reconstruction.






