Background
Breast reconstruction entered the modern era when Hartrampf, Scheflan, and Black introduced the transverse rectus abdominis myocutaneous (TRAM) flap in 1982. [1] This ingenious procedure reliably transfers autogenous tissue for reconstruction and has the added benefit of abdominal rejuvenation. The TRAM flap has proven to be the autogenous tissue of choice for breast reconstruction. [2, 3]
The main advantage of the procedure lies in the consistency of the reconstructed breast; it is similar to the natural breast in softness and in the way the tissue drapes on the chest. Because the tissue is part of the patient's body, it does not incite foreign-body reaction or capsular contractures, which have plagued implant reconstructions. Furthermore, since scars fade and tissues soften, the reconstruction only improves over time, which is not true of implant reconstructions.
Since the inception of the TRAM flap, surgeons have developed different methods to improve blood supply to the transferred abdominal tissues. These methods currently include use of a midabdominal TRAM flap, a bipedicled TRAM flap, a microvascular augmentation (supercharge) of a unipedicled TRAM flap, a "delay" of a unipedicled TRAM flap, [4] and a free-tissue transfer (or free) TRAM flap, which includes perforator flaps. Of these procedures, only the free TRAM flap takes full advantage of the primary blood supply (inferior epigastric blood vessels) of the TRAM flap tissues. This technique completely removes the abdominal tissues from the body and transplants them to the chest area.
A diagram is shown below.
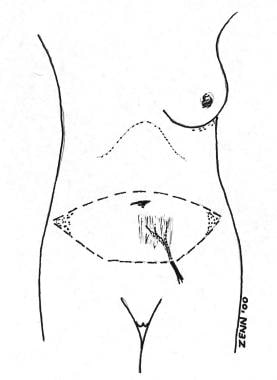 Diagram of the blood supply to the free transverse rectus abdominis myocutaneous (TRAM) flap. Note that the deep inferior epigastric vessels supply the flap, the primary blood supply to the lower abdomen. The shaded areas of the flap are discarded.
Diagram of the blood supply to the free transverse rectus abdominis myocutaneous (TRAM) flap. Note that the deep inferior epigastric vessels supply the flap, the primary blood supply to the lower abdomen. The shaded areas of the flap are discarded.
The blood supply is furnished by microscopic reconnection of the inferior epigastric artery and vein(s) at the mastectomy site. While this procedure is more technically exacting and formidable compared with other TRAM techniques, experienced microsurgeons routinely perform free-tissue transfers with success rates of more than 98% at most centers. When performed properly in the properly selected patient, the free TRAM flap procedure may produce a breast reconstruction superior to that of any other technique.
Epidemiology
Frequency
This procedure recently accounted for approximately 20% of breast reconstructions performed in the United States.
Indications
Consider free TRAM flap reconstruction for any patient undergoing mastectomy, either as an immediate procedure (at the time of mastectomy) or as a delayed procedure (some time after mastectomy). Simultaneous bilateral breast reconstruction may be performed with 2 free TRAM flaps. The patient must be psychologically motivated and have adequate tissues in the abdominal area to be considered for a free TRAM flap. Implant reconstruction and tissue reconstruction may be considered for any patient, though the following relative indications favor the free TRAM flap procedure.
-
Division of the superior epigastric blood supply by previous surgery, making a pedicled TRAM flap impossible
-
Radical mastectomy defect with large tissue requirement
-
History of radiation to the chest wall
-
Large opposite breast (difficult to match with an implant)
-
Small opposite breast (difficult to match with an implant)
-
Previous failure of implant reconstruction
-
Excess lower abdominal tissue and patient desires abdominoplasty
-
Desire to have the maximum possible blood supply to the TRAM tissues [6]
Relevant Anatomy
The flap skin and fat of a free TRAM flap reconstruction survive on perforators through the rectus abdominis muscle. Although this muscle has a dual blood supply (ie, the superior and inferior epigastric arteries), this operation relies only on the inferior epigastric arterial system. Since this is the primary blood supply of these tissues, excellent vascularity is noted over most of the TRAM flap, even in tissue not directly adjacent to the muscle perforators. Only a small cuff of rectus abdominis muscle is harvested with the flap, thereby limiting dissection of the abdominal wall and postoperative discomfort.
In patients with favorable anatomy, all muscle can be preserved and only the perforating vessels are taken with the flap (so-called perforator flaps). If the primary vessels used are the deep inferior epigastric artery and vein, the flap is called a deep inferior epigastric perforator (DIEP) flap. [8] If the primary vessels used are the superficial inferior epigastric artery and vein, the flap is called a superficial inferior epigastric perforator (SIEP) flap.
Because ultimate abdominal discomfort and function can be similar for patients after operations involving traditional free TRAM flaps and perforator flaps, some microsurgeons do not believe the added operative time and risk of dissecting only the perforators are indicated. However, data suggest less abdominal morbidity and lower requirements for pain management for the perforator flap patient. In the final analysis, the type of free-tissue transfer performed depends on the patient's desires and anatomy and the surgeon's experience and preference. [8, 9, 10]
Contraindications
The free TRAM flap operation is major surgery and should not be undertaken lightly by the patient or surgeon. Fifteen years' experience with these procedures enables the author to identify the following characteristics that place patients at higher risk for complications:
-
Cardiac disease (ie, myocardial infarction, angina, congestive heart failure)
-
Pulmonary disease (ie, emphysema, chronic obstructive pulmonary disease)
-
History of pulmonary embolus or deep venous thrombosis
-
Collagen-vascular disease, lupus, scleroderma, polyarteritis (small-vessel disease)
-
Unstable psychiatric disease
-
Obesity (>25% above ideal body weight)
-
Age (physiologic age >70 y) [11]
-
Previous surgery that has interrupted blood supply to the TRAM flap
-
Previous surgery, irradiation, or anatomy that is unfavorable to harvesting the tissues or that makes reconnection at the recipient site impossible (often can be determined only at the time of surgery)
-
Contraindication(s) to anticoagulation therapy
Because of the magnitude of the procedure and the degree of stress on the lungs and heart, this operation may unmask baseline cardiopulmonary disease and result in a complicated postoperative course. In addition, anything that causes small-vessel disease, such as the medical conditions listed above or cigarette smoking, may cause complications in the transferred tissue and in the abdominal donor site. Any of the above characteristics contraindicate a TRAM flap procedure; in such cases, the surgeon should seek another method of reconstruction.
-
Diagram of the blood supply to the free transverse rectus abdominis myocutaneous (TRAM) flap. Note that the deep inferior epigastric vessels supply the flap, the primary blood supply to the lower abdomen. The shaded areas of the flap are discarded.
-
Patient 1. This patient has small breasts and has a small amount of abdominal tissue available. This is the perfect indication for a free transverse rectus abdominis myocutaneous (TRAM) flap to maximize the amount of tissue available for reconstruction.
-
Patient 1. Postoperative view. Note the natural ptosis of the reconstruction and the distinct inframammary fold, not distorted by a muscle pedicle from the abdomen. The patient does not desire nipple-areolar reconstruction.
-
Patient 2. This patient has a large opposite breast to match and does not desire a breast reduction. A free transverse rectus abdominis myocutaneous (TRAM) flap allows a large block of tissue to be transferred, matching the opposite breast.
-
Patient 2. Postoperative view. The breast envelope has been filled with the free transverse rectus abdominis myocutaneous (TRAM) flap. Note the abdominal improvement, an added benefit of the TRAM procedure. The patient still requires nipple-areolar reconstruction.
-
Patient 3. Preoperative markings. The patient has a large opposite breast and does not desire breast reduction. Note the large amount of skin that will be removed. A free transverse rectus abdominis myocutaneous (TRAM) allows a large reconstruction to match the opposite side.
-
Patient 3. Postoperative view. There is a good volume match, and the resected breast skin has been replaced with abdominal skin.
-
Patient 3. Postoperative view. In this view, note the natural droop of the reconstruction, unobtainable with breast implants. All of the patient's scars are below her tan lines.






