Practice Essentials
Gynecomastia is derived from the Greek terms gynec (feminine) and mastos (breast). The literal translation, male breasts, relates to any condition that results in excessive development of breast tissue in males. Males may rarely develop breast cancer, but this is often associated with testicular atrophy. [1]
Male breast volume is composed of a combination of ductal and stromal tissue, commonly referred to as glandular tissue, and an increase in adipocytes, typically referred to as fatty tissue. Excess skin resulting in significant ptosis of the breast may be present in patients with severe gynecomastia. See the images below.
 Preoperative gynecomastia patient. Note the enlarged breast size. Courtesy of Jay Pensler, MD.
Preoperative gynecomastia patient. Note the enlarged breast size. Courtesy of Jay Pensler, MD.
 Postsurgical correction of gynecomastia. Note the improved contour, which enables the patient to look better both in and out of clothes. Courtesy of Jay Pensler, MD.
Postsurgical correction of gynecomastia. Note the improved contour, which enables the patient to look better both in and out of clothes. Courtesy of Jay Pensler, MD.

 Postoperative view of above patient. Note that while the glandular and fatty tissue have been removed, the nipples remain in the preoperative position relative to each other. Also note the significant skin retraction postoperatively.
Postoperative view of above patient. Note that while the glandular and fatty tissue have been removed, the nipples remain in the preoperative position relative to each other. Also note the significant skin retraction postoperatively.

 Postoperative view of patient after surgical glandular excision and combined ultrasonic-assisted liposuction (UAL) and power-assisted liposuction (PAL). Courtesy of Jay Pensler, MD.
Postoperative view of patient after surgical glandular excision and combined ultrasonic-assisted liposuction (UAL) and power-assisted liposuction (PAL). Courtesy of Jay Pensler, MD.
Workup in gynecomastia
Longstanding, stable cases in adults do not require blood tests other than those that would be required for an outpatient surgery. Blood work should include liver function tests and assays for follicle-stimulating hormone, luteinizing hormone, human chorionic gonadotropin, thyroid-stimulating hormone, thyroxine, estrogen, estradiol, and testosterone levels in children and in individuals with progressive disease.
A sex chromatin study should be performed to exclude Klinefelter syndrome when appropriate.
If indicated by the patient's history, physical examination, and laboratory results, preoperative workup may include the following:
-
Ultrasonographic examination of the testes and breasts
-
Computed tomography (CT) scanning of the adrenal glands
-
Magnetic resonance imaging (MRI) of the sella turcica
-
Mammography
Excisional biopsy or fine-needle aspiration of breast tissue should be performed if a breast tumor is suspected.
Histologically, gynecomastia has three recognized pathologic patterns, as follows [2] :
-
Florid type - Characterized by an increase in the number and length of ducts, proliferation of ductal epithelium, periductal edema, a highly cellular fibroblastic stroma and hypervascularity, and the formation of pseudolobules
-
Fibrous type - Characterized by dilated ducts with minimal proliferation of epithelium, an absence of periductal edema, and an almost acellular fibrous stroma without adipose tissue
-
Intermediate type - An overlapping pattern of the florid and fibrous types
Management of gynecomastia
Surgical therapy for gynecomastia includes the following:
-
Surgical resection (subcutaneous mastectomy) - The most common approach is the intra-areolar incision, or Webster incision
-
Two-stage breast reduction - For moderate-to-severe gynecomastia; the first stage is liposuction followed by a Webster-type periareola incision and removal of gland, fat, and fibrous tissue to obtain a nice contour; the second stage is performed 4-6 months later, after the blood supply has reestablished itself from below and allows for a periareola donut mastopexy
-
Minimally invasive gynecomastia surgery - A very small (approximately 5 mm) incision is made at the areolar edge, and liposuction is followed by release of the glandular tissue from the overlying areola, with the tissue then pulled through the incision
-
Liposuction-assisted mastectomy
History of the Procedure
Galen introduced the term gynecomastia in the second century AD. He defined gynecomastia as an unnatural increase in the breast fat of males. Although Galen was aware that glandular enlargement of the male breast occurred as a separate entity, he did not consider this gynecomastia.
The first recorded description of a reduction mammaplasty was by Paulas of Aegina in the seventh century AD, who referred to the condition as an "effeminacy of men." Several medical and surgical treatments of gynecomastia were described in the 1800s.
Treatment of gynecomastia has continued to evolve over the ages. Presently, a multifaceted surgical approach is used to optimize correction of the deformity. The fatty component is removed with one or a combination of the variants of liposuction, while the glandular component requires direct excision. The skin is redraped over the underlying structures or, in severe cases, resected. The patient's treatment plan should be crafted to correct the specific problems that are unique to his specific case. [3, 4, 5]
Problem
Gynecomastia results in an increase in breast tissue in males that, when problematic, is readily detectable by other individuals. The increased tissue may be breast glandular tissue, adipose (fatty) in nature, or a combination of the two. This results in significant functional and psychological limitations. The physical deformation may also be exquisitely painful. As a general rule, the glandular tissue is significantly more painful than the fatty tissue. Situations like gym class may require children or adolescents to remove their shirts in the presence of other students. This can put a boy with gynecomastia in danger not only of embarrassment but also of physical harm.
Most patients have never heard of this condition until the family physician identifies it. The physician may be unaware of the possible causes of the condition and its psychological impact. After initial presentation, boys are frequently advised to ignore the gynecomastia and are told that it will go away. Fortunately, in most instances, cases of minimal subareolar pubertal-onset gynecomastia do regress as puberty progresses.
Individuals with no regression or even progression of the deformity often receive little or no understanding about the shame and humiliation they experience. Coaches, sergeants, physicians, parents, and peers (both boys and girls) can inflict damage out of ignorance, cruelty, or both. The author reports that a parent recently exclaimed during an initial evaluation, "I just don't understand why 'he' has to slouch around all the time." Postural and clothing modifications to mask the deformity are the norm in these patients from puberty through adulthood.
Awareness of gynecomastia needs to progress in order to inform the men and boys with gynecomastia and their physicians what can be done to improve the condition.
Epidemiology
Frequency
Gynecomastia can occur in persons of any age. During adolescence, males develop firmness around the breast as the breast bud enlarges due to the hormonal fluxes of puberty. The subareolar firmness which normally develops regresses with time. Breast tissue is typically present on a microscopic level in male patients; a small amount of breast tissue is normal. The visible appearance of breast tissue in a male is abnormal.
The definition of clinically significant gynecomastia is subject to interpretation by any author; therefore, reports in the literature are often confusing, as the reader is forced to compare apples to oranges when examining different studies. Nydick et al reported 65% of boys "may have the problem" but cautioned that it typically resolves. [6] Webster noted the incidence of gynecomastia to be around 8% in a series of naval patients, [7] while Williams noted that 40% of men examined in his series of autopsies had gynecomastia to some degree. [8] Approximately 40% of healthy men and up to 70% of hospitalized men have palpable if not visible breast tissue. The incidence of some degree of palpable breast tissue in males increases to more than 60% in those in the seventh decade of life in one series.
Etiology
Gynecomastia can be classified based on etiology. Idiopathic gynecomastia accounts for over 85% of cases that require surgical intervention.
Physiologic gynecomastia occurs primarily in newborns and in adolescents at puberty. In the newborn, the neonatal breast results from the action of maternal estrogens, placental estrogens, or both in concert. The increased breast tissue usually disappears in a few weeks. Neonatal gynecomastia is not a problem that requires surgical intervention.
Adolescent gynecomastia, by definition, is initiated during puberty. The median age of onset is 13 years. Breast tissue growth is often asymmetrical, and the breasts are frequently tender. Adolescent gynecomastia usually regresses by the latter teen years. Note that the normal course during puberty is for a palpable, often visible, mass below the areola that begins to resolve in the mid teen years. While continued visible enlargement in the size of the breast is not normal in a teenager, residual palpable gynecomastia may be present in one or both breasts through the mid teen years. The authors would stress that the norm would be progressive diminution of any visible or palpable deformity through this period. In each case, the clinician must evaluate the degree of tissue present, the clinical presentation, and the physical and psychological effects on the patient.
Pathologic gynecomastia may be due to testosterone deficiency, increased estrogen production, or increased conversion of androgens to estrogens. The pathologic conditions associated with gynecomastia include congenital anorchia, Klinefelter syndrome, [9] testicular feminization, hermaphroditism, adrenal tumors, liver disorders, pituitary tumors, and malnutrition.
Many pharmacological agents have been linked to gynecomastia. [10] These drugs can be categorized by their mechanisms of action. The first type is drugs that act exactly like estrogens (eg, diethylstilbestrol, birth control pills, digitalis, estrogen-containing cosmetics). The second type is drugs that enhance endogenous estrogen formation (eg, gonadotropins, progesterone, clomiphene). The third type is drugs that inhibit testosterone synthesis and action (eg, ketoconazole, metronidazole, and cimetidine). The final type is drugs that act by unknown mechanisms (eg, isoniazid, [11] methyldopa, captopril, tricyclic antidepressants, diazepam, marijuana, heroin). While heavy marijuana use has been linked to gynecomastia in rats, the relationship in humans is at best poorly documented. Chronic alcohol abuse may result in hepatocellular destruction and scarring which may result in gynecomastia. Adult patients should be routinely questioned about alcohol abuse or addiction.
A link between testicular atrophy, Klinefelter syndrome, and breast cancer has been noted. Longstanding, stable gynecomastia in an otherwise healthy male does not require an extensive medical workup.
Pathophysiology
In boys, the main sex hormone is testosterone, which is secreted by the testes. In girls, the main sex hormone is estrogen, which is secreted by the ovaries. However, both hormones are secreted in both sexes. Some production of estrogen occurs in the testes, and some production of testosterone occurs in the ovaries. Gynecomastia has long been considered the result of an imbalance between estrogens, which stimulate breast tissue, and androgens, which antagonize this effect. An alteration in the normal ratio of estrogen to androgen has been found in patients with gynecomastia in association with many different etiological factors. [12, 13]
Estradiol is the growth hormone of the breast in women, and an excess of estradiol leads to the proliferation of breast tissue. Under normal circumstances, most estradiol in men is derived from the peripheral conversion of testosterone and adrenal estrogen. The basic mechanisms of physiologic gynecomastia have been postulated to represent a decrease in androgen production, an absolute increase in estrogen production, and an increased availability of estrogen precursors for peripheral conversion to estradiol. See the image below.
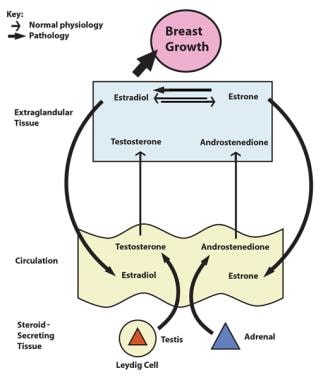 Pathophysiology of gynecomastia. Estradiol is the growth hormone of the breast, and an excess of estradiol leads to the proliferation of breast tissue. Under normal circumstances, most estradiol in men is derived from the peripheral conversion of testosterone and adrenal estrone. The basic mechanism of endocrine-related gynecomastia is a decrease in androgen production, an absolute increase in estrogen production, and an increased availability of estrogen precursors for peripheral conversion to estradiol.
Pathophysiology of gynecomastia. Estradiol is the growth hormone of the breast, and an excess of estradiol leads to the proliferation of breast tissue. Under normal circumstances, most estradiol in men is derived from the peripheral conversion of testosterone and adrenal estrone. The basic mechanism of endocrine-related gynecomastia is a decrease in androgen production, an absolute increase in estrogen production, and an increased availability of estrogen precursors for peripheral conversion to estradiol.
The etiology of most cases of gynecomastia remains unknown. The number of breast malignancies does not appear to be increased in patients with idiopathic gynecomastia. Patients who present with gynecomastia and have Klinefelter syndrome do exhibit an increased incidence of breast malignancies. Pensler et al noted that patients with Klinefelter syndrome exhibited elevated estrogen and progesterone receptors in their breast tissue. [14] The presence of elevated estrogen and progesterone receptors in patients with Klinefelter syndrome provides a potential mechanism by which these patients may develop breast neoplasms. By contrast, patients with idiopathic gynecomastia did not demonstrate an increased number of estrogen or progesterone receptors. Also, the binding affinity of the receptors in both groups were not affected. The absence of elevated progesterone or estrogen receptors in patients with idiopathic gynecomastia helps to explain why these patients rarely manifest breast malignancy.
Presentation
Patients present with an increase in breast tissue, which is asymmetrical in one third of cases. The degree of asymmetry between the two sides varies widely. [15] Some patients present with unilateral gynecomastia, while other individuals have a size discrepancy between the two sides that ranges from moderate to severe. Breast tenderness may also be noted in one third of patients. Enlargement is usually central and symmetrical, although occasionally it is eccentric.
In 1934, Webster classified gynecomastia into 3 types. [7] The first is glandular. Patients with a glandular component require surgical removal of the gland. The second is fatty glandular. With the fatty glandular form, surgery combined with liposuction allows good contouring. The third is simple fatty. In the cases that are primarily fatty in nature, liposuction alone provides good results.
Another classification described by Simon in 1973 groups the patients into categories according to the size of the gynecomastia. [16] Group 1 is minor but visible breast enlargement without skin redundancy. Group 2A is moderate breast enlargement without skin redundancy. Group 2B is moderate breast enlargement with minor skin redundancy. Group 3 is gross breast enlargement with skin redundancy that simulates a pendulous female breast. Patients in groups 1 and 2 require no skin excision, but the breast development associated with group 3 is so marked that excess skin must be removed.
Indications
Generally, gynecomastia is a benign condition. Longstanding cases do not require histologic examination of surgically removed tissue. Rapid changes in the size of the breast, especially when unilateral in nature, may represent a malignancy particularly when pharmacologic manipulation can be ruled out. Also, changes in breast size in a patient with Klinefelter syndrome should be viewed with caution.
Surgical intervention is indicated in patients for diagnostic purposes or, most commonly, for patients who request treatment for physical modification. Most patients who visit a plastic surgeon request treatment for improvement of the obvious physical deformity which enhances psychological and physical well-being. These patients seek treatment because they find that the condition, which is readily apparent in everyday life, adversely impacts day-to-day activities under various circumstances. The physical deformation necessitates behavioral modifications that have numerous implications in the lives of the patients who are affected. Patients wear loose clothing and often avoid exposure in showers and swimming pools. Patients in high school and college are reticent to participate in any athletic activity that may directly or inadvertently require removal of one's shirt, exposing the chest.
Patients with gynecomastia typically slouch forward and roll the shoulders toward the midline in an effort to camouflage the deformation. The aforementioned posturing has a submissive connotation to the public with whom they interact. Patients return for postoperative appointments standing tall. In cases involving teenagers, parents typically remark "I have been trying to have him stand up straight for years!" The postural changes alone, which result at all age levels both sitting and standing, have numerous positive implications in peer-to-peer interactions. The confidence a patient gains after surgery becomes a life-changing event.
A study by Innocenti et al suggested that the reason patients undergo gynecomastia surgery and their level of satisfaction with the operation vary with body type. The report involved adult patients classified according to one of three different body types—high muscle mass, normal, or overweight—who were treated with subcutaneous mastectomy. The investigators found that the primary reason patients with normal body type underwent surgery was emotional distress owing to a feminine chest appearance. In contrast, most of those with high muscle mass wanted the operation because unsatisfactory contouring of the pectoralis area had damaged their self-confidence, while the majority of patients in the overweight group underwent surgery because they looked upon gynecomastia as a weight disorder. The study also found that patients with normal body type had higher levels of satisfaction with their surgical outcomes than did members of the other two groups. [17]
Relevant Anatomy
The plastic surgeon must be familiar with the anatomy of the breast and be able to differentiate between the fat (adipose) tissue and the glandular tissue. In a liposuction-assisted mastectomy, the surgeon primarily targets the fatty component of the breast. The glandular tissue is quite dense and is extremely resistant to removal by any method other than direct excision. All patients have a glandular component and a fatty component. The requirement of direct surgical resection of glandular tissue in patients may explain the poor results obtained by some inexperienced practitioners in specific cases. As previously mentioned, longstanding stable cases of gynecomastia do not routinely require histological examination of the excised tissue.
See the images below.
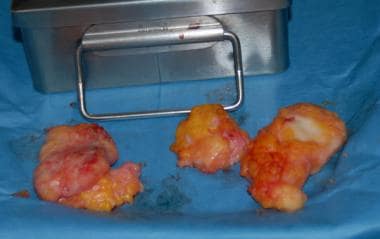 Resected tissue. Note that the white tissue, which is glandular breast tissue, has a higher density than the fat (adipose) tissue. The thick and dense glandular tissue is not amenable to liposuction.
Resected tissue. Note that the white tissue, which is glandular breast tissue, has a higher density than the fat (adipose) tissue. The thick and dense glandular tissue is not amenable to liposuction.
Contraindications
Liposuction-assisted mastectomy with or without gland excision for gynecomastia patients can be performed under local anesthesia, intravenous conscious sedation, or general anesthesia. The choice of sedation should be determined preoperatively by the physician and patient. Any significant medical problems, such as heart disease, lung disease, or diabetes, must be excluded before the procedure is performed. Rapid or unusual progression or presentation of the disease may require endocrinologic evaluation, which is optimally preformed prior to any surgical intervention. If the etiology of the gynecomastia is related to an adrenal or pituitary tumor, the tumor should be addressed prior to any attempt to correct the gynecomastia. If the gynecomastia is related to drug use, the use of the offending agent should be stopped prior to surgery.
Males who are upset with the appearance of their chest may also have substantial psychological issues. A boy who is being abused or humiliated commonly focuses on some part of his external appearance to avoid dealing with internal pain that he feels unable to manage or control. What may have started as a minor physical condition can be a cover for much deeper emotional issues that no amount of surgery can resolve. While Yost has demonstrated that more than 91% of individuals who have had surgery are happy with the procedure and would recommend surgery to a friend, individuals who require multiple surgeries may need to be screened for body dysmorphic disorder (BDD) and referred for treatment. [18]
-
Pathophysiology of gynecomastia. Estradiol is the growth hormone of the breast, and an excess of estradiol leads to the proliferation of breast tissue. Under normal circumstances, most estradiol in men is derived from the peripheral conversion of testosterone and adrenal estrone. The basic mechanism of endocrine-related gynecomastia is a decrease in androgen production, an absolute increase in estrogen production, and an increased availability of estrogen precursors for peripheral conversion to estradiol.
-
Flow chart of the workup to determine the etiology of gynecomastia.
-
Incision for minimally invasive gynecomastia surgery.
-
The Webster intra-areolar incision is placed in the inferior hemisphere.
-
The Webster intra-areolar incision may be enlarged by lateral and medial extensions.
-
The transverse nipple-areola incision.
-
A periareola incision followed by another outer circle of skin. The skin in between is removed and the outer circle has a purse-string closure, which is approximated to the smaller circle. This completes the peiareola donut mastopexy.
-
The most common technique for skin resection and nipple transposition is the Letterman technique.
-
In massive gynecomastia, an en bloc resection of excessive skin and breast tissue and free nipple grafting can be performed using an elliptical incision with a nipple-areola graft.
-
Stage 2 - Periareola skin excision with a purse-string closure.
-
Preoperative anteroposterior view of a patient with idiopathic gynecomastia.
-
Preoperative lateral view of a patient with gynecomastia.
-
Postoperative view of above patient. Note that while the glandular and fatty tissue have been removed, the nipples remain in the preoperative position relative to each other. Also note the significant skin retraction postoperatively.
-
Postoperative view of patient after surgical glandular excision and combined ultrasonic-assisted liposuction (UAL) and power-assisted liposuction (PAL). Courtesy of Jay Pensler, MD.
-
Preoperative gynecomastia patient. Note the enlarged breast size. Courtesy of Jay Pensler, MD.
-
Postsurgical correction of gynecomastia. Note the improved contour, which enables the patient to look better both in and out of clothes. Courtesy of Jay Pensler, MD.
-
Resected tissue. Note that the white tissue, which is glandular breast tissue, has a higher density than the fat (adipose) tissue. The thick and dense glandular tissue is not amenable to liposuction.
-
Preoperative view. Note the excess tissue in the axillary region in addition to the tissue in the breast. Treatment in addition to correction of the gynecomastia requires aggressive liposuction of the axilla. Courtesy of Jay Pensler, MD.
-
Postoperative view of above patient. Note the correction not only of the gynecomastia but the improved transition into the axilla (armpit). Courtesy of Jay Pensler, MD.
-
Preoperative gynocomastia patient. Courtesy of Jay Pensler, MD.
-
Postsurgical correction of gynecomastia. Gland excision with liposuction. Note the large mole on the right chest that has flattened out. Courtesy of Miguel Delgado, MD.
-
Preoperative gynecomastia patient. Courtesy of Miguel Delgado, MD.
-
Postsurgical correction of gynecomastia. Gland excision with liposuction. Note how the skin contracts. Courtesy of Miguel Delgado, MD.
-
Resected gynecomastia tissue. Courtesy of Miguel Delgado, MD.
-
Pull-through technique. Tissue seen pulled half way through the incision. Preoperative and postoperative photos of this patient. Courtesy of Miguel Delgado, MD.
-
Preoperative photo before the pull-through technique. Courtesy of Miguel Delgado, MD.
-
Glandular tissue being pulled through. Courtesy of Miguel Delgado, MD.
-
Breast gland pulled through from each side. Courtesy of Miguel Delgado, MD.
-
Postoperative photo after pull through technique. Courtesy of Miguel Delgado, MD.
-
Thirteen-year-old with adolescent gynecomatia. Gland excision with liposuction only, no skin excision. Note the degree of skin contraction. A secondary periareola-skin resection could remove the small fold. Courtesy of Miguel Delgado, MD.
-
Twenty-five-year-old with adolescent gynecomastia. Courtesy of Miguel Delgado, MD.
-
Postoperative photo after gland excision and liposuction. Patient is seen 6 month after surgery. Courtesy of Miguel Delgado, MD.
-
Forty-eight-year-old male gynecomastia patient with breast ptosis. Courtesy of Miguel Delgado, MD.
-
Three months postoperative after a superior cresant lift, triple-V incision. Note how the areola is elevated so the inframammary fold nearly eliminated. Courtesy of Miguel Delgado, MD.
-
Fifteen-year-old boy with severe gynecomastia. Courtesy of Miguel Delgado, MD.
-
Postoperative photo after stage 1 gland excision and liposuction through a Webster incision. Note the significant contraction of the skin, but laxity is still present. Courtesy of Miguel Delgado, MD.
-
Postoperatively, after periareola donut mastopexy. Patient seen 3 months after sugery. The skin laxity has been improved. Courtesy of Miguel Delgado, MD.
-
Forty-five-year-old man with adolescent gynecomastia. Courtesy of Miguel Delgado, MD.
-
Postoperative hematoma. The most common complication in the coauthor's practice. Courtesy of Miguel Delgado, MD.
-
Patient seen 2 months after evacuation of hematoma. If the hematoma is treated appropriately (ie, immediately removed), there will be no long-term ill effects. Courtesy of Miguel Delgado, MD.
-
A 16-year-old patient with adolescent gynecomastia. Courtesy of Jay Pensler, MD.
-
Postoperative view of the adolescent gynecomastia patient at 8 months after surgery. Note the improved profile and the contraction of the skin envelope as a result of the glandular tissue removal. Courtesy of Jay Pensler, MD.
-
Preoperative view of a male aged 32 years with bilateral gynecomastia. Note the excess skin present prior to surgery.
-
Postoperative view of the patient from the previous image. Extensive skin undermining and redraping were needed to achieve the demonstrated result.





