Background
Glutathione synthetase (GS) deficiency, first described in 1970, is a rare autosomal-recessive inborn error of glutathione metabolism characterized by severe metabolic acidosis, hemolytic anemia, and neurological problems. [1, 2, 3, 4] Biochemical findings include massive excretion of 5-oxoproline in the urine. In mild glutathione synthetase deficiency, which is characterized by hemolytic anemia, enzyme deficiency primarily occurs in erythrocytes. See the image below.
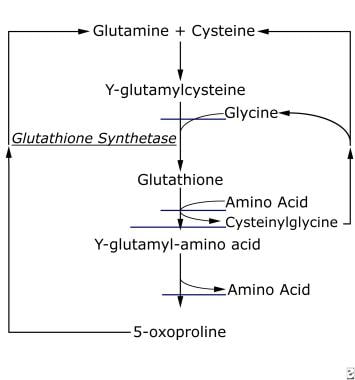 Biochemical pathway of glutathione synthetase.
Biochemical pathway of glutathione synthetase.
Pathophysiology
Glutathione is involved in several important biologic functions, including membrane transport, detoxification of xenobiotics, and protection of cells from free radicals. Glutathione is produced from the amino acids cysteine, glycine, and glutamine via the consecutive actions of gamma-glutamylcysteine synthetase and glutathione synthetase. It is also widely used by RBCs, which are vulnerable to oxidative damage caused by peroxides. Reduced glutathione is required as an antioxidant in these cases.
Multiple mutations that cause glutathione synthetase deficiency have been described in the glutathione synthetase gene, GSS. The erythrocyte variant has been linked to a homozygous missense mutation that causes enzyme instability; thus, enzyme deficiency is most significant in erythrocytes and manifests as hemolytic anemia. Thirteen different missense mutations in GSS have been identified in individuals with severe glutathione synthetase deficiency. [5] The mutations were found in 9 unrelated patients from different geographic areas. Two of these mutations were in individuals who were found to have CNS involvement. In all cases, residual enzyme activity was noted, indicating that a complete loss of enzyme function is probably lethal.
Epidemiology
Frequency
United States
The frequency of glutathione synthetase deficiency is unknown.
International
Glutathione synthetase deficiency is very rare. Worldwide, only approximately 40-50 cases in which the patient survived the newborn period have been published. The overall frequency is unknown. It is believed that some cases of glutathione synthetase deficiency may go undiagnosed or misdiagnosed, complicating a determination of its true frequency.
Mortality/Morbidity
Recently, authors have recommended that 3 forms of glutathione synthetase deficiency be identified: mild, moderate, and severe (see History). In the severe systemic form, chronic metabolic acidosis must be managed. Long-term prognosis is guarded. With careful treatment during infancy, many patients survive, and the metabolic acidosis may become more manageable after infancy. The lack of glutathione in erythrocytes alone is apparently tolerable, as has been noted with the mild form of this condition; however, in severe glutathione synthetase deficiency, a progressive loss of function occurs, leading to severe intellectual disability, ataxia, and seizure disorders.
According to one review, the oldest reported survivor with the severe form of glutathione synthetase deficiency was aged 24 years and had experienced significant neurological deterioration over the previous few years. Psychotic behavior, tremors, and dysarthria have also been reported. Patients with the moderate or mild forms have been reported to have long-term survival and little or no neurological sequelae.
Race
No race predilection is observed in glutathione synthetase deficiency.
Sex
No sex predilection is known in glutathione synthetase deficiency.
Age
Most individuals with systemic glutathione synthetase deficiency are diagnosed in the newborn period. However, with the isolated erythrocyte form, the diagnosis may not be made until adulthood, although hemolytic anemia is present at birth.
-
Biochemical pathway of glutathione synthetase.







