Practice Essentials
Enterobiasis (also known as pinworm infestation) is caused by the small nematode Enterobius vermicularis. (See the image below.) This common helminthic infestation has an estimated prevalence of 40 million infected individuals in the United States. [1] The female nematode averages 10 mm × 0.7 mm, whereas males are smaller. All socioeconomic levels are affected. Infestation often occurs in family clusters. Infestation does not equate with poor home sanitary measures (an important point when discussing therapy).

Signs and symptoms of enterobiasis
Patients are often asymptomatic. Pinworms may be incidentally discovered when they are seen in the perineal region. If patients are symptomatic, pruritus ani and pruritus vulvae are common presenting symptoms.
See Presentation for more detail.
Diagnosis of enterobiasis
Eggs are usually deposited in great quantities on the perineum at night. The diagnosis is made by identifying eggs under the low-power lens of a microscope.
See Workup for more detail.
Management of enterobiasis
An antihelminthic medication should be prescribed to patients with pinworm infestation. Application of an antipruritic ointment or albendazole may help control itching and scratching. [2]
Thorough handwashing can deter transmission.
See Treatment and Medication for more detail.
Pathophysiology
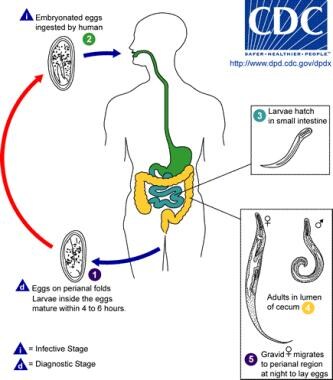
E vermicularis is an obligate parasite; humans are the only natural host. Fecal-oral contamination via hand-mouth contact or via fomites (toys, clothes) are common methods of infestation. After ingestion, eggs usually hatch in the duodenum within 6 hours. Worms mature in as little as 2 weeks and have a life span of approximately 2 months.
Adult worms normally inhabit the terminal ileum, cecum, vermiform appendix, and proximal ascending colon. The worms live free in the intestinal lumen. Little evidence supports invasion of healthy tissue under normal conditions. The female worm migrates to the rectum after copulation and, if not expelled during defecation, migrates to the perineum (often at night) where an average of 11,000 eggs are released. Eggs become infectious within 6-8 hours and, under optimum conditions, remain infectious in the environment for as long as 3 weeks.
See the image below.
 Because of the short incubation time until the ova are infectious, eggs that are deposited under the fingernails during scratching and then placed in the mouth may be a mode of reinfestation.
Because of the short incubation time until the ova are infectious, eggs that are deposited under the fingernails during scratching and then placed in the mouth may be a mode of reinfestation.
Epidemiology
United States statistics
Prevalence is approximately 5-15% in the general population; however, this rate has declined in recent years. Prevalence rates are probably higher in institutionalized individuals. Humans are the only known host.
Infestation rate increases with increased population density, and with personal habits such as thumb sucking
International statistics
E vermicularis infestation occurs worldwide. Prevalence data vary by country.
A study that aimed to determine the extent of enterobiasis, strongyloidiasis, and other helminth infections in infants, preschool-aged, and school-aged children from rural coastal Tanzania reported that E vermicularis infestations were found in 4.2% of infants, 16.7%, of preschool-aged children, and 26.3% of school-aged children. [3]
A study of kindergarten students in the Republic of the Marshall Islands found that the overall prevalence of E vermicularis infestation was 22.4%. The prevalence was higher among boys (24.5%) than among girls (20.31%) in the study. [4]
Infestation rates increase with increased population density and with certain personal habits like thumb-sucking. [5, 6]
Race-, sex-, and age-related demographics
All races are subject to infestation.
Infestation can occur in males and females.
The people most likely to be infected with pinworms are children younger than 18 years, people who take care of infected children, and people who are institutionalized. In these groups, the prevalence can reach 50%. [1] However, individuals can be affected regardless of age or health status.
Prognosis
The prognosis is excellent, but reinfestation is common.
Morbidity/mortality
Secondary bacterial skin infection may develop from vigorous scratching to relieve pruritus. Reinfestation is common. Infection can develop as long as female pinworms continue to lay eggs on the skin. Restless sleeping may be due to pruritus ani. Infestation has been reported to cause enuresis.
Immunocompromised hosts
Although other helminthic infection rates are shown to be higher in patients with HIV, studies to date have not shown a statistically significant difference for E vermicularis. [7]
Complications
Beware of skin infection from vigorous scratching to relieve pruritus.
Pinworms have been associated with appendicitis, [8, 9] nocturnal vaginal discharge, [10] and inflammation of the female genital tract. [10] However, small and large intestine ulcerations, perianal abscesses, intestinal pain, transient synovitis, and enuresis are believed to be coincidental and not causal. [11]
If a patient with enterobiasis is refractory to treatment, consider the possibility of an infestation with Dipylidium caninum, which is a common tapeworm that infects domestic cats and dogs. [12]
Patient Education
Inform families that dogs and cats do not harbor E vermicularis.
Inform families that infestation may occur in spite of proper child and household hygiene.
Counsel families to avoid overreaction through aggressive sanitary measures. Because infectious eggs may be in bedclothes and dust and remain infectious for 20 days, wet-mopping floors or vacuuming carpets and washing bedclothes are prudent precautions.
Reassuring families that pinworms are not a sexually transmitted disease and are not evidence of child abuse may be helpful.
Keeping the patient's fingernails trimmed to prevent excoriations is helpful.
Avoid scratching the area and nail biting because this is a cause of autoinfection.
Encourage the patient to bathe in the morning; this significantly reduces the number of eggs.
Children may return to school once they have received a dose of medication, bathed, and have nails trimmed.
Bed linens should be washed in hot, soapy water.
-
Because of the short incubation time until the ova are infectious, eggs that are deposited under the fingernails during scratching and then placed in the mouth may be a mode of reinfestation.
-
Pinworms in a young patient.






