Tappe D, Zidowitz S, Demmer P, Kern P, Barth TF, Frosch M. Three-dimensional reconstruction of Echinococcus multilocularis larval growth in human hepatic tissue reveals complex growth patterns. Am J Trop Med Hyg. 2010 Jan. 82(1):126-7. [QxMD MEDLINE Link]. [Full Text].
Jenkins EJ, Peregrine AS, Hill JE, Somers C, Gesy K, Barnes B, et al. Detection of European Strain of Echinococcus multilocularis in North America. Emerg Infect Dis. 2012 Jun. 18(6):1010-2. [QxMD MEDLINE Link]. [Full Text].
Shabbir MU, Ahmed A, Shaukat F, et al. Disseminated hydatid disease in a child involving multiple organ systems: a case report. Cureus. 2020 Jan 4. 12 (1):e6564. [QxMD MEDLINE Link].
Balen Topić M, Skuhala T, Desnica B, Višković K, Drinković M. Repeated percutaneous treatment of massive hepatic cystic echinococcosis in a child. Pediatrics. 2018 Dec. 142 (6):[QxMD MEDLINE Link].
Bristow BN, Lee S, Shafir S, Sorvillo F. Human echinococcosis mortality in the United States, 1990-2007. PLoS Negl Trop Dis. 2012. 6(2):e1524. [QxMD MEDLINE Link]. [Full Text].
Himsworth CG, Jenkins E, Hill JE, Nsungu M, Ndao M, Andrew Thompson RC. Emergence of sylvatic Echinococcus granulosus as a parasitic zoonosis of public health concern in an indigenous community in Canada. Am J Trop Med Hyg. 2010 Apr. 82(4):643-5. [QxMD MEDLINE Link]. [Full Text].
Wahlers K, Menezes CN, Wong ML, Zeyhle E, Ahmed ME, Ocaido M. Cystic echinococcosis in sub-Saharan Africa. Lancet Infect Dis. 2012 Nov. 12(11):871-80. [QxMD MEDLINE Link].
Piarroux M, Piarroux R, Knapp J, Bardonnet K, Dumortier J, Watelet J, et al. Populations at risk for alveolar echinococcus, France. Emerg Infect Dis. May 2013. 19(5):721-728.
Schneider R, Gollackner B, Schindl M, Tucek G, Auer H. Echinococcus canadensis G7 (pig strain): an underestimated cause of Cystic Echinococcosis in Austria. Am J Trop Med Hyg. 2010 May. 82(5):871-4. [QxMD MEDLINE Link]. [Full Text].
Nothdurft HD, Jelinek T, Mai A, et al. [Epidemiology of echinococcosis in Bavaria]. Dtsch Med Wochenschr. 1995 Aug 25. 120(34-35):1151-5. [QxMD MEDLINE Link].
Midyat L, Gökçe S, Onder A, Ozdemir Y, Mursalov G, Mir S. A very rare cause of childhood paraparesis: primary intradural extramedullary spinal hydatid cyst. Pediatr Infect Dis J. 2009 Aug. 28(8):754-5. [QxMD MEDLINE Link].
Rosenblatt JE. Laboratory diagnosis of infections due to blood and tissue parasites. Clin Infect Dis. 2009 Oct 1. 49(7):1103-8. [QxMD MEDLINE Link].
Salant H, Abbasi I, Hamburger J. The development of a loop-mediated isothermal amplification method (LAMP) for Echinococcus granulosis coprodetection. Am J Trop Med Hyg. 2012 Nov. 87(5):883-7. [QxMD MEDLINE Link]. [Full Text].
Kern P. Clinical features and treatment of alveolar echinococcosis. Curr Opin Infect Dis. 2010 Oct. 23(5):505-12. [QxMD MEDLINE Link].
Pérez-Molina JA, Díaz-Menéndez M, Gallego JI, Norman F, Monge-Maillo B, Ayala AP, et al. Evaluation of nitazoxanide for the treatment of disseminated cystic echinococcosis: report of five cases and literature review. Am J Trop Med Hyg. 2011 Feb. 84(2):351-6. [QxMD MEDLINE Link].
Ammann RW, Eckert J. Cestodes. Echinococcus. Gastroenterol Clin North Am. 1996 Sep. 25(3):655-89. [QxMD MEDLINE Link].
Golemanov B, Grigorov N, Mitova R, Genov J, Vuchev D, Tamarozzi F. Efficacy and Safety of PAIR for Cystic Echinococcosis: Experience on a Large Series of Patients from Bulgaria. Am J Trop Med Hyg. 2011 Jan. 84(1):48-51. [QxMD MEDLINE Link].
Salinas JL, Gonzales HV, Astuvilca J, Arce-Villavicencio Y, Carbajal-Gonzalez D, Talledo L, et al. Long-term albendazole effectiveness for hepatic cystic echinococcosis. Am J Trop Med Hyg. 2011 Dec. 85(6):1075-9. [QxMD MEDLINE Link].
García MB, Lledías JP, Pérez IG, Tirado VV, Pardo LF, Bellvís LM. Primary Super-Infection of Hydatid Cyst--Clinical Setting and Microbiology in 37 Cases. Am J Trop Med Hyg. 2010 Mar. 82(3):376-378. [QxMD MEDLINE Link]. [Full Text].
Li Y, Zheng H, Cao X, Liu Z, Chen L. Demographic and clinical characteristics of patients with anaphylactic shock after surgery for cystic echinococcosis. Am J Trop Med Hyg. 2011 Sep. 85(3):452-5. [QxMD MEDLINE Link].
Li Y, Zheng H, Gu M, Cao X, Wen H, Liu Z, et al. Comparisons of Serum Total IgE, IgG, and IgG1 Levels in Patients with and without Echinococcosis-Induced Anaphylactic Shock. Am J Trop Med Hyg. 2012 Jul. 87(1):104-108. [QxMD MEDLINE Link].
Schneider R, Aspock H, Auer H. Unexpected increase of alveolar echinococcosis, Austria, 2012. Emerg Infect Dis. March 2013. 19(3):475-477.
Lederer W, Wiedermann FJ, Bale R. Pericyst radiofrequency ablation treatment for hepatic alveolar echinococcosis: a case report and review of the literature. Infect Dis Clin Pract. May 2012. 20(3):177-179.
Agarwal N, Kumar S. Budd-Chiari syndrome owing to liver hydatid disease: case report and review of the literature. Ann Trop Paediatr. 2009 Dec. 29(4):301-4. [QxMD MEDLINE Link].
American Academy of Pediatrics. Other tapeworm infections (including hydatid disease). Red Book: 2009 Report of the Committee on Infectious Diseases. 28th. Elk Grove Village, IL: American Academy of Pediatrics; 2009. 654-5.
Arandes AS, Bertomeu FG, Artero JM. Microscopic image of the protoscolex of Echinococcus granulosus on the "Hydatid Sand". Am J Trop Med Hyg. 2010 Jun. 82(6):980. [QxMD MEDLINE Link].
Hydatid Disease. Spector JM, Gibson TE. Atlas of Pediatrics in the Tropics and Resource-Limited Settings. Elk Grove Village, IL: American Academy of Pediatrics; 2009. 113-117.
Barth TF, Herrmann TS, Tappe D, Stark L, Grüner B, Buttenschoen K, et al. Sensitive and specific immunohistochemical diagnosis of human alveolar echinococcosis with the monoclonal antibody Em2G11. PLoS Negl Trop Dis. 2012. 6(10):e1877. [QxMD MEDLINE Link]. [Full Text].
Ben Nouir N, Nunez S, Gianinazzi C, et al. Assessment of Echinococcus granulosus somatic protoscolex antigens for serological follow-up of young patients surgically treated for cystic echinococcosis. J Clin Microbiol. 2008 May. 46(5):1631-40. [QxMD MEDLINE Link].
Bordier Affinity Products SA. Echinococcus multilocularis: ELISA kit for the diagnosis of alveolar echinococcosis in humans. Bordier Affinity Products. Available at http://www.bordier.ch/echinomultilo/.
Brunetti E, Garcia HH, Junghanss T. Cystic echinococcosis: chronic, complex, and still neglected. PLoS Negl Trop Dis. 2011 Jul. 5(7):e1146. [QxMD MEDLINE Link]. [Full Text].
Brunetti E, Junghanss T. Update on cystic hydatid disease. Curr Opin Infect Dis. 2009 Oct. 22(5):497-502. [QxMD MEDLINE Link].
Brunetti E, White AC Jr. Cestode infestations: hydatid disease and cysticercosis. Infect Dis Clin North Am. 2012 Jun. 26(2):421-35. [QxMD MEDLINE Link].
Capan M, Keltner S, Thalhammer F, Winkler S, Jäger W, Zeitlinger M. Intra-cystic drug concentration of albendazole sulphoxide in patients with Echinococcus granulosus cysts. Am J Trop Med Hyg. 2009 Oct. 81(4):712-3. [QxMD MEDLINE Link].
CDC. Alveolar Hydatid Disease. Centers for Disease Control and Prevention. Available at http://www.cdc.gov/ncidod/dpd/parasites/alveolarhydatid/default.htm.
CDC. Identification and Diagnosis of Parasites of Public Health: Echinococcus. Centers for Disease Control and Prevention. Available at http://www.dpd.cdc.gov/dpdx/html/Echinococcosis.htm.
Craig P. Echinococcus multilocularis. Curr Opin Infect Dis. 2003 Oct. 16(5):437-44. [QxMD MEDLINE Link].
Craig PS, McManus DP, Lightowlers MW, et al. Prevention and control of cystic echinococcosis. Lancet Infect Dis. 2007 Jun. 7(6):385-94. [QxMD MEDLINE Link].
D'Alessandro A, Rausch RL. New aspects of neotropical polycystic (Echinococcus vogeli) and unicystic (Echinococcus oligarthrus) echinococcosis. Clin Microbiol Rev. 2008 Apr. 21(2):380-401, table of contents. [QxMD MEDLINE Link].
Demir HA, Demir S, Emir S, Kacar A, Tiryaki T. Primary hydatid cyst of the rib mimicking chest wall tumor: a case report. J Pediatr Surg. 2010 Nov. 45(11):2247-9. [QxMD MEDLINE Link].
Dervenis C, Delis S, Avgerinos C, Madariaga J, Milicevic M. Changing concepts in the management of liver hydatid disease. J Gastrointest Surg. 2005 Jul-Aug. 9(6):869-77. [QxMD MEDLINE Link].
Dincer SI, Demir A, Sayar A, et al. Surgical treatment of pulmonary hydatid disease: a comparison of children and adults. J Pediatr Surg. Jul 2006. 41(7):1230-6. [QxMD MEDLINE Link].
Djuricic SM, Grebeldinger S, Kafka DI, Djan I, Vukadin M, Vasiljevic ZV. Cystic echinococcosis in children - the seventeen-year experience of two large medical centers in Serbia. Parasitol Int. 2010 Jun. 59(2):257-61. [QxMD MEDLINE Link].
Durakbasa CU, Tireli GA, Sehiralti V, et al. An audit on pediatric hydatid disease of uncommon localization: incidence, diagnosis, surgical approach, and outcome. J Pediatr Surg. 2006 Aug. 41(8):1457-63. [QxMD MEDLINE Link].
Eckert J, Deplazes P. Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin Microbiol Rev. 2004 Jan. 17(1):107-35. [QxMD MEDLINE Link].
Elmali M, Ceyhan M, Ilgar M, Koprulu C, Ozfindik M, Sancak R. Hepatic hydatid cyst rupture and anaphylaxis after a fall. Indian J Pediatr. 2009 Mar. 76(3):329-30. [QxMD MEDLINE Link].
Elshazly AM, Awad SE, Hegazy MA, Mohammad KA, Morsy TA. Echinococcosis granulosus/hydatidosis an endemic zoonotic disease in Egypt. J Egypt Soc Parasitol. 2007 Aug. 37(2):609-22. [QxMD MEDLINE Link].
Ermis F, Dursun M, Akyuz F, Bakir B, Guven K. Hydatid cysts: three different stages on the same image. Intern Med. 2007. 46(19):1673. [QxMD MEDLINE Link].
Findikcioglu A, Kilic D, Canpolat T, Hatipoglu A. Primary hydatid disease of the chest wall. Ann Thorac Cardiovasc Surg. 2007 Jun. 13(3):203-5. [QxMD MEDLINE Link].
Garcia HH, Moro PL, Schantz PM. Zoonotic helminth infections of humans: echinococcosis, cysticercosis and fascioliasis. Curr Opin Infect Dis. 2007 Oct. 20(5):489-94. [QxMD MEDLINE Link].
Guzel A, Tatli M, Maciaczyk J, Altinors N. Primary cerebral intraventricular hydatid cyst: a case report and review of the literature. J Child Neurol. 2008 May. 23(5):585-8. [QxMD MEDLINE Link].
Gümüs M, Yagmur Y, Gümüs H, Kapan M, Onder A, Böyük A. Primary hydatid disease of diaphragm with subcutenous extension. J Infect Dev Ctries. 2011 Aug 12. 5(8):599-602. [QxMD MEDLINE Link].
Hemama M, Lasseini A, Rifi L, Boutarbouch M, Derraz S, Ouahabi AE, et al. A sacral hydatid cyst mimicking an anterior sacral meningocele. J Neurosurg Pediatr. 2011 Nov. 8(5):526-9. [QxMD MEDLINE Link].
Hesse AA, Nouri A, Hassan HS, Hashish AA. Parasitic infestations requiring surgical interventions. Semin Pediatr Surg. 2012 May. 21(2):142-50. [QxMD MEDLINE Link].
Hidron A, Vogenthaler N, Santos-Preciado JI, Rodriguez-Morales AJ, Franco-Paredes C, Rassi A Jr. Cardiac involvement with parasitic infections. Clin Microbiol Rev. 2010 Apr. 23(2):324-49. [QxMD MEDLINE Link].
Horton J. Albendazole: a broad spectrum anthelminthic for treatment of individuals and populations. Curr Opin Infect Dis. 2002 Dec. 15(6):599-608. [QxMD MEDLINE Link].
Ibrahim BB, Haridy FM, Hegazi MM, Morsy TA. Human hydatidosis granulosus in greater Cairo, Egypt: with general review. J Egypt Soc Parasitol. 2007 Aug. 37(2):681-8. [QxMD MEDLINE Link].
Ito A, Nakao M, Sako Y. Echinococcosis: serological detection of patients and molecular identification of parasites. Future Microbiol. 2007 Aug. 2:439-49. [QxMD MEDLINE Link].
Ito A, Wandra T, Sato MO, Mamuti W, Xiao N, Sako Y. Towards the international collaboration for detection, surveillance and control of taeniasis/ cysticercosis and echinococcosis in Asia and the Pacific. Southeast Asian J Trop Med Public Health. 2006. 37 Suppl 3:82-90. [QxMD MEDLINE Link].
Kalkan E, Cengiz SL, Ciçek O, Erdi F, Baysefer A. Primary spinal intradural extramedullary hydatid cyst in a child. J Spinal Cord Med. 2007. 30(3):297-300. [QxMD MEDLINE Link].
Kjossev KT, Losanoff JE. Classification of hydatid liver cysts. J Gastroenterol Hepatol. 2005 Mar. 20(3):352-9. [QxMD MEDLINE Link].
Knapp J, Chirica M, Simonnet C, Grenouillet F, Bart JM, Sako Y, et al. Echinococcus vogeli Infection in a Hunter, French Guiana. Emerg Infect Dis. 2009 Dec. 15(12):2029-31. [QxMD MEDLINE Link].
Kosar A, Orki A, Haciibrahimoglu G, et al. Effect of capitonnage and cystotomy on outcome of childhood pulmonary hydatid cysts. J Thorac Cardiovasc Surg. 2006 Sep. 132(3):560-4. [QxMD MEDLINE Link].
Kumar VA, Mehta A, Agara D. Actively motile larval forms in fluid aspirated from lung. Hydatid cyst of the lung. Clin Infect Dis. 2010 Oct 1. 51(7):804-5, 865-6. [QxMD MEDLINE Link].
Kurkcuoglu IC, Eroglu A, Karaoglanoglu N, et al. Surgical approach of pulmonary hydatidosis in childhood. Int J Clin Pract. 2005 Feb. 59(2):168-72. [QxMD MEDLINE Link].
Kuzucu A, Soysal O, Ozgel M, Yologlu S. Complicated hydatid cysts of the lung: clinical and therapeutic issues. Ann Thorac Surg. Apr 2004. 77(4):1200-4. [QxMD MEDLINE Link].
Mahmood Nouriyan S, Mokhtari M, Abbasi Fard S, Nouriyan N. Primary solitary hydatid cyst in paraspinal cervical muscles: a case report and review of the literature. Neurol Neurochir Pol. 2011 Jul-Aug. 45(4):387-90. [QxMD MEDLINE Link].
Mandell GL. Cestodes (tapeworms). Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases. 5th ed. Philadelphia, Pa: Churchill Livingstone; 2005. 3285-93.
Mata-Miranda P, Osnaya-Palma I, Rodriguez-Prado U, et al. Epidemiologic and ultrasonographic study of echinococcosis in a community in the state of Mexico. Am J Trop Med Hyg. 2007 Sep. 77(3):500-3. [QxMD MEDLINE Link].
Mavridis G, Livaditi E, Christopoulos-Geroulanos G. Management of hydatidosis in children. Twenty-one year experience. Eur J Pediatr Surg. 2007 Dec. 17(6):400-3. [QxMD MEDLINE Link].
McManus DP, Zhang W, Li J, Bartley PB. Echinococcosis. Lancet. Oct 18 2003. 362(9392):1295-304. [QxMD MEDLINE Link].
Mishra PK, Agrawal A, Joshi M, Sanghvi B, Gupta R, Parelkar SV. Minimal access surgery for multiorgan hydatid cysts. Afr J Paediatr Surg. 2010 Jan-Apr. 7(1):40-2. [QxMD MEDLINE Link].
Molavipour A, Javan H, Moghaddam AA, Dastani M, Abbasi M, Ghahramani S. Combined medical and surgical treatment of intracardiac hydatid cysts in 11 patients. J Card Surg. 2010 Mar. 25(2):143-6. [QxMD MEDLINE Link].
Moringlane ILG. Echinococcus spp. Akuffo H, Linder E, Ljungstrom I, Wahlgren M. Parasites of the Colder Climates. London and New York: Taylor & Francis; 2003. 177-183.
Moro P, Schantz PM. Cystic echinococcosis in the Americas. Parasitol Int. 2006. 55 Suppl:S181-6. [QxMD MEDLINE Link].
Moro P, Schantz PM. Echinococcosis: a review. Int J Infect Dis. 2009 Mar. 13(2):125-33. [QxMD MEDLINE Link].
Neuville M, Grisoli D, Nicoud A, Jacquier A, Lagier JC, Collart F. Cardiac hydatidosis. Am J Trop Med Hyg. 2010 Jul. 83(1):102-3. [QxMD MEDLINE Link].
Ozturk G, Aydinli B, Yildirgan MI, et al. Posttraumatic free intraperitoneal rupture of liver cystic echinococcosis: a case series and review of literature. Am J Surg. 2007 Sep. 194(3):313-6. [QxMD MEDLINE Link].
Pandey A, Arya CL, Asthana AK. Pulmonary hydatidosis: an unusual cause of haemoptysis. Indian J Med Microbiol. 2007 Apr. 25(2):158-60. [QxMD MEDLINE Link].
Reiter-Owona I, Grüner B, Frosch M, Hoerauf A, Kern P, Tappe D. Serological confirmatory testing of alveolar and cystic echinococcosis in clinical practice: results of a comparative study with commercialized and in-house assays. Clin Lab. 2009. 55(1-2):41-8. [QxMD MEDLINE Link].
Richter J, Orhun A, Grüner B, Müller-Stöver I, Reuter S, Romig T, et al. Autochthonous cystic echinococcosis in patients who grew up in Germany. Euro Surveill. 2009 Jun 4. 14(22):[QxMD MEDLINE Link].
Santivanez S, Garcia HH. Pulmonary cystic echinococcosis. Curr Opin Pulm Med. 2010 May. 16(3):257-61. [QxMD MEDLINE Link].
Sapkas GS, Machinis TG, Chloros GD, et al. Spinal hydatid disease, a rare but existent pathological entity: case report and review of the literature. South Med J. Feb 2006. 99(2):178-83. [QxMD MEDLINE Link].
Schantz PM. Progress in diagnosis, treatment and elimination of echinococcosis and cysticercosis. Parasitol Int. 2006. 55 Suppl:S7-S13. [QxMD MEDLINE Link].
Sekmenli T, Koplay M, Sezgin A. Isolated omental hydatid cyst: clinical, radiologic, and pathologic findings. J Pediatr Surg. 2009 May. 44(5):1041-3. [QxMD MEDLINE Link].
Smego RA Jr, Sebanego P. Treatment options for hepatic cystic echinococcosis. Int J Infect Dis. 2005 Mar. 9(2):69-76. [QxMD MEDLINE Link].
Thompson RC. The taxonomy, phylogeny and transmission of Echinococcus. Exp Parasitol. 2008 Aug. 119(4):439-46. [QxMD MEDLINE Link].
Tolan RW, Turcios NL. Pulmonary echinococcosis. Infect Dis Pract. 2006. 30:493-5.
Vasilopoulou V, Makris A, Mostrou G, Spoulou V, Syriopoulou V, Theodoridou M. A 2-year-old girl with fever, abdominal pain, and lung cavities. Pediatr Infect Dis J. 2010 Nov. 29(11):1061, 1065-6. [QxMD MEDLINE Link].
Vasquez JC, Montesinos E, Peralta J, Rojas L, DeLaRosa J, Leon JJ. Need for lung resection in patients with intact or ruptured hydatid cysts. Thorac Cardiovasc Surg. 2009 Aug. 57(5):295-302. [QxMD MEDLINE Link].
Voros D, Katsarelias D, Polymeneas G, et al. Treatment of hydatid liver disease. Surg Infect (Larchmt). 2007 Dec. 8(6):621-7. [QxMD MEDLINE Link].
Yalcin E, Kiper N, Tan C, et al. The role of human leucocyte antigens in children with hydatid disease: their association with clinical condition and prognosis. Parasitol Res. 2010 Mar. 106(4):795-800. [QxMD MEDLINE Link].
Yeola-Pate M, Banode PJ, Bhole AM, et al. Different locations of hydatid cysts: case illustration and review of literature. Infect Dis Clin Pract. Nov 2008. 16:379-84.
Youn H. Review of zoonotic parasites in medical and veterinary fields in the Republic of Korea. Korean J Parasitol. 2009 Oct. 47 Suppl:S133-41. [QxMD MEDLINE Link]. [Full Text].
Zhang W, Li J, McManus DP. Concepts in immunology and diagnosis of hydatid disease. Clin Microbiol Rev. 2003 Jan. 16(1):18-36. [QxMD MEDLINE Link]. [Full Text].
Echinococcosis. World Health Organization. Available at http://www.who.int/mediacentre/factsheets/fs377/en/#. May 2015; Accessed: July 20, 2015.
Parasites - Echinococcosis. Centers for Disease Control and Prevention. Available at http://www.cdc.gov/parasites/echinococcosis/prevent.html. December 12, 2012; Accessed: July 20, 2015.
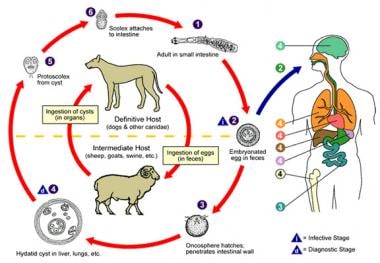 Diagram of the Echinococcus life cycle, provided by the Centers for Disease Control and Prevention.
Diagram of the Echinococcus life cycle, provided by the Centers for Disease Control and Prevention.


