Practice Essentials
Abnormal uterine bleeding (AUB), an updated term for the condition often referred to as dysfunctional uterine bleeding (DUB), is classically defined as excessively heavy, prolonged, or frequent bleeding of uterine origin that is not caused by pregnancy or recognizable pelvic or systemic disease. [1, 2] It usually results from disordered functioning of the hypothalamic-pituitary-ovarian (HPO) axis and is often associated with anovulatory cycles. [3] This classic definition highlights that anovulatory uterine bleeding (as part of the etiologic spectrum of AUB) is a diagnosis of exclusion.
AUB occurs most often in the beginning and end of the reproductive years: 20% of cases occur in adolescent females, and as many as 50% of women aged 40-50 years experience AUB (see Abnormal [Dysfunctional] Uterine Bleeding and Abnormal [Dysfunctional] Uterine Bleeding in Emergency Medicine). Of these cases of AUB, about 90% are due to menstrual periods when ovulation does not occur. Adolescent females have several anovulatory cycles per year; hence, anovulatory uterine bleeding is the primary cause of AUB in the female adolescent population. [4, 5, 6]
In 2011, a revised terminology system for AUB in nongravid reproductive-age women was introduced by the International Federation of Gynecology and Obstetrics (FIGO). The FIGO classified AUB according to the PALM-COEIN system, in which the acronym PALM represents structural causes (polyps, adenomyosis, leiomyomas, malignancy and hyperplasia) and the acronym COEIN represents nonstructural causes (coagulopathy, ovulatory dysfunction, endometrial, iatrogenic, and not yet classified). [7]
In this system, AUB is further qualified by adding a suffix reflecting the cause of the abnormal bleeding. For example, AUB from ovulatory dysfunction is designated as AUB-O. In addition, AUB can be categorized as either AUB/heavy menstrual bleeding (HMB [8] ; ie, what has been commonly referred to as menorrhagia) or AUB/intermenstrual bleeding (IMB; ie, metrorrhagia). [9, 10]
The FIGO system was reviewed, clarified, and, where necessary, revised in late 2018; however, the fundamental structure of the system remained. [11]
It has been suggested that the term DUB should be retired and that AUB, appropriately qualified as described above, should be used instead. However, a number of medical authors have continued to use the term DUB.
Management must be tailored to the condition of each patient. For most patients, treatment consists of oral contraceptive pills (OCPs) and iron supplementation. Standard practice is that only patients with acute severe hemorrhage require more intensive treatment.
Patients with AUB who do not respond to medical therapy may require endometrial curettage, hysteroscopic evaluation, or both. In life-threatening circumstances where medical therapy is ineffective or contraindicated, endometrial ablation or hysterectomy may be the only reasonable alternative.
Pathophysiology
The normal menstrual cycle, characterized by sequential growth, maturation, and eventual sloughing of the endometrial mucosa, is produced by the cyclic release of estrogen and progesterone from the ovary. This process (orchestrated by the HPO axis) occurs with amazing regularity throughout most of a woman's reproductive lifetime.
An understanding of the normal cyclic fluctuations of the two gonadotropins (ie, luteinizing hormone [LH] and follicle-stimulating hormone [FSH]) and the primary female reproductive hormones (ie, estrogen and progesterone) helps clarify the hormonal abnormalities associated with anovulation. [12]
The first 14 days of a typical 28-day menstrual cycle (day 1 being defined as the first day of menstrual flow) are characterized by rising FSH levels, which stimulate ovarian follicle development and the subsequent production of estrogens (primarily estradiol). Serum progesterone levels are extremely low during this stage. LH levels climb more slowly but abruptly peak on day 12 or 13 in positive response to rising estrogen levels. (See the image below.)
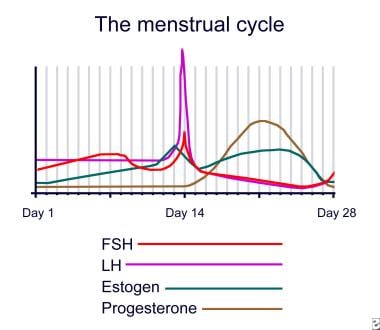 Menstrual cycle.
Menstrual cycle.
During that first 14-day period, the endometrium, under the influence of estrogen, undergoes proliferation. The LH surge stimulates ovulation (on or about day 14) and conversion of the ovulatory follicle to a corpus luteum, which is responsible for estrogen and progesterone production. Under the influence of this progesterone, the endometrium is converted to a secretory state in preparation for implantation, if fertilization of the ovum should occur. Progesterone is produced only if ovulation occurs.
As LH levels drop (on the assumption that fertilization and production of human chorionic gonadotropin [HCG] by the developing conceptus did not occur), the corpus luteum regresses, estrogen and progesterone levels plummet, and the endometrium deteriorates and is sloughed.
The average menstrual cycle is 28-29 days (range, 21-35 d). Initially, some teenagers can have cycles as long as 45 days. Over time, the menstrual cycle becomes fairly consistent from month to month in any given woman. Normal menstrual flow lasts for 7 days or less and produces an average total blood loss of 25-69 mL. Women who experience (1) bleeding either more frequently than every 21 days or less frequently than every 45 days, (2) a menstrual flow longer than 7 days, and (3) blood loss exceeding 80 mL are considered to have abnormal menstrual cycles.
With anovulation, estrogen levels rise as usual in the early phase of the cycle. In the absence of ovulation, a corpus luteum never forms, and progesterone is not produced. The endometrium moves into a hyperproliferative state, ultimately outgrowing its estrogen supply. This leads to irregular sloughing of the endometrium and excessive bleeding from spiral arteries that have not undergone physiologic senescence.
Etiology
Anovulation can result from dysfunction from any pathway of the HPO axis. In the pediatric age group, the vast majority of cases can be attributed to an immature HPO axis with acyclic hormonal stimulation of the endometrium. Although anovulatory bleeding can occur in any female of reproductive age, the following female patients may be at greater risk for AUB:
-
Adolescents during the first 3-5 years following menarche
-
Patients with eating disorders (eg, anorexia nervosa or bulimia)
-
Adolescents with a body mass index (BMI) higher than 30 (>95% for age in the obesity range)
-
Adolescents experiencing significant psychological stress
-
Athletes with significant exercise stress [13]
COVID-19 vaccines have been associated with menstrual irregularities and menorrhagia; however, the effects on the menstrual cycle are generally well tolerated and transient, with symptoms typically resolving within about 2 months. [14]
Epidemiology
United States and international statistics
The exact incidence of AUB is unknown. In the United States, the epidemiologic basis consists of case series reports from tertiary institutions citing female patients who most likely do not reflect the general population. Nearly 50% of all women have irregular periods in the first year after menarche; and of these, more than 50% of the cycles are anovulatory. Irregular periods can persist for as long as 5 years after menarche in 20% of women. [15]
International rates should reflect those seen in the US.
Age- and race-related demographics
Worldwide, the age of menarche varies and is influenced by female biology, genetic factors, and environmental factors. Geographic region, race, and ethnicity also play significant roles. The median age of menarche worldwide has been declining, but the magnitude of the decline has been subject to contention.
In the United States, the average age of menarche has been reported to be 11.9 years. [16] In Canada [17] and the United Kingdom, [18] the average ages of menarche have been reported to be 12.7 years and 12.3 years, respectively. Irregular and anovulatory cycles may persist for 1-5 years after menarche; however, regulation of menstrual periods typically occurs within 2 years.
Race does not contribute significantly to the incidence of AUB.
Prognosis
Overall, adolescents with AUB have an excellent prognosis, with most outgrowing the problem within 3-5 years of menarche. Compliant patients for whom oral contraceptive pills are prescribed rarely have recurrent episodes of AUB. For patients with AUB related to systemic disease, the prognosis depends upon the underlying disease process.
Patient Education
The patient and her caregivers should be educated about the normal menstrual cycle and the generally benign nature of AUB. It is a good idea for her to record a calendar history of her menstrual cycles, noting the beginning and end dates of bleeding. The patient should be advised to return if she experiences (1) bleeding more frequently than every 21 days or less frequently than every 45 days, (2) a menstrual flow longer than 7 days, and (3) overall blood loss exceeding 80 mL (~5 tbsp), or if she cannot comply with the prescribed outpatient treatment.
For patient education resources, see the Women's Health Center, as well as Vaginal Bleeding, Amenorrhea, Anemia, and Painful Ovulation (Mittelschmerz).
-
Menstrual cycle.





