Practice Essentials
Acute respiratory distress syndrome (ARDS) continues to contribute significantly to the disease burden in today’s arena of pediatric critical care medicine. It is an acute, diffuse, inflammatory lung injury caused by diverse pulmonary and nonpulmonary etiologies. Pathophysiology is characterized by increased vascular permeability, increased lung weight, and loss of aerated tissue within 7 days of insult. Hypoxemia, new pulmonary opacities (unilateral or bilateral) on chest imaging, decreased lung compliance, and increased physiological dead space are telltale clinical signs. See the image below. Diffuse alveolar damage characterized by edema, inflammation, hyaline membrane formation, or pulmonary hemorrhage is the pathological hallmark. [1, 2, 3]
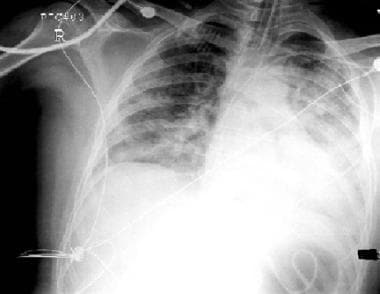 Chest radiograph in 3-year-old girl who developed acute respiratory distress syndrome due to overwhelming gram-negative sepsis. Salient features include endotracheal tube; diffuse, bilateral infiltrates; air bronchograms on left side; and central venous catheter. Ratio of arterial oxygen tension to fraction of inspired oxygen at time of chest radiography was 100.
Chest radiograph in 3-year-old girl who developed acute respiratory distress syndrome due to overwhelming gram-negative sepsis. Salient features include endotracheal tube; diffuse, bilateral infiltrates; air bronchograms on left side; and central venous catheter. Ratio of arterial oxygen tension to fraction of inspired oxygen at time of chest radiography was 100.
The taxonomy of ARDS has evolved over the decades. The most recent definition was outlined by a panel of 56 pediatric experts known as the Pediatric Acute Lung Injury Consensus Conference (PALICC-2) Group in 2023. [3] The most recently updated pediatric ARDS (PARDS) definition is as follows.
Definition
Age: Perinatal lung diseases are excluded.
Onset: Within 7 days of pulmonary or nonpulmonary insult.
Origin of pulmonary edema: It should be noncardiogenic pulmonary edema and not fully explainable by fluid overload.
Chest imaging: Showing new-onset unilateral or bilateral pulmonary opacities excluding atelectasis or effusion. The opacities are representative of acute parenchymal lung disease.
Oxygenation impairment: Identified as partial pressure of oxygen/fraction of inspired oxygen (PaO2/FiO2 or P/F) ratio ≤ 300, oxygen saturation (SpO2)/FiO2 (S/F) ≤ 250, oxygenation index (OI) ≥ 4, or oxygen saturation index (OSI) ≥ 5. The calculations of the P/F and S/F ratio, OI, and OSI are included later in this chapter. The presence of a full face mask with positive end-expiratory pressure (PEEP) of at least 5 is essential for the diagnosis of PARDS for the patient receiving full face mask noninvasive ventilation (NIV).
Special populations: The same diagnostic criteria can be applied to special populations, including children with cyanotic heart disease (CHD) and chronic lung disease (CLD). In this special population, worsening hypoxemia should not be fully explainable by worsening heart conditions.
Disease stratification: This can be applied after initial 4 hours of establishing the diagnosis of PARDS. It is based on the degree of oxygenation impairment, as follows:
-
Mild to moderate PARDS: P/F ratio of 101-300, S/F ratio of 151-250, OI of 4-16, OSI of 5-12
-
Severe PARDS: P/F ratio of ≤ 100, S/F ≤ 150, OI ≥ 16, OSI ≥ 12
Please note that this disease stratification cannot be applied to the special population with CHD and CLD.
Possible PARDS and at risk for ARDS
The new guidelines also include a discussion about patients with possible PARDS and those at risk for PARDS. Pediatric patients receiving high-flow nasal cannula (HFNC) or nasal NIV can be diagnosed to have possible PARDS if they meet the rest of the PARDS criteria of age group, disease onset, chest imaging, and oxygen threshold. Those without chest imaging but otherwise meeting the rest of the criteria will also fall into the PARDS category. Children receiving respiratory support with any interface requiring supplemental oxygen to maintain SpO2 > 88%, but not meeting the criteria of PARDS or possible PARDS, are considered at risk for PARDS. The definition of supplemental oxygen includes FiO2 > 21% on invasive mechanical ventilation; or FiO2 > 21% on NIV; or for those receiving oxygen flow from a mask or cannula that exceeds these age-specific thresholds: ≥ 2 L/min (age < 1 yr), ≥ 4 L/min (age 1-5 yr), ≥ 6 L/min (age 6-10 yr), or ≥ 8 L/min (age > 10 yr). For children on a mask or cannula, oxygen flow is calculated as FiO2 × flow rate (L/min) (eg, 10 L/min flow at 0.35 FiO2 = 3.5 L/min). [3]
Overview of PARDS management
After the establishment of these new definitions, the committee also created guidelines for PARDS management, which are included in the guidelines. In a nutshell, a utilization of low tidal volume (4-8 mL/kg of predicted body weight) using the PEEP/FiO2 table, limiting plateau pressure to 28 cm H2O (32 if reduced chest wall compliance), and a permissive hypoxemia and hypercapnia strategy has been discussed. Definite recommendations were not provided for or against the use of prone positioning, high-frequency oscillatory ventilators (HFOV), and recruitment maneuvers. The use of corticosteroids is recommended in selected populations only. The committee recommended against the use of surfactant. Meticulous consideration of inhaled nitric oxide therapy is recommended in severe ARDS cases and in cases bridging to extracorporeal life support (ECLS). [2, 3]
The details of each treatment component are included in the Treatment section, and a summary of PALICC-2 recommendations is included in the Guidelines section.
Background
The discussion of ARDS is incomplete without appreciating historic work by Ashbaugh and colleagues, who were first to describe the concept of ARDS in 1967. They presented eleven adults and one pediatric patient who suffered from acute onset of tachypnea and hypoxemia refractory to supplemental oxygen. The authors also discussed the benefits of PEEP for the management of atelectasis and a plausible role of corticosteroids in certain cases. The loss of lung compliance was noted clinically, and pulmonary inflammation, edema, and hyaline membrane formation were seen on autopsy. These observations were significant and remain indispensable even after 48 years. [4]
ARDS was referred to as adult respiratory distress syndrome in some of the studies. [5] But now it is consistently known as acute respiratory distress syndrome (ARDS), because it is a well-known entity in pediatric population since the first description in 1967. [4] In the past 5 decades, our knowledge and experience have grown substantially, and the definition continues to evolve. The American-European Consensus Conference (AECC) definition of ARDS was published in 1994 [6, 7] and had certain limitations that were addressed 17 years later by Berlin definition in 2012. [1] The PALICC group made their first set of recommendations relevant to the pediatric population in 2015. [2] This was followed by a second set of recommendations in 2023. [3]
The oxygen indices used in PARDS definitions can be calculated with the following equations:
- The PaO2/FiO2 (P/F) ratio can be calculated using PaO2 in mm of Hg and FiO2 in decimals from 0.21 to 1.0.
- Oxygenation index (OI) = (FiO2 × mean airway pressure × 100)/PaO2
- Oxygen saturation index (OSI) = FiO2 × mean airway pressure × 100/SPO2
For example, a patient receiving mechanical ventilation with a mean airway pressure of 20 cm H2O, FiO2 of 0.6 has SPO2 of 98% and PaO2 of 85 mm Hg.
OI = (0.6 × 20 × 100)/85 = 14.11
OSI = (0.6 × 20 × 100)/98 = 12.24
P/F ratio = 85/0.6 = 141.66
This patient has moderate ARDS.
Please note that a patient needs to have an arterial line to measure PaO2, as it represents the partial pressure of oxygen in the arterial blood. For those who do not have an arterial line, the S/F ratio and OSI should be calculated.
Go to Acute Respiratory Distress Syndrome and Barotrauma and Mechanical Ventilation for complete information on these topics.
Pathophysiology
ARDS follows a cascade of events after direct pulmonary or systemic insult resulting in the disruption of the alveolar-capillary unit. The pathophysiology of ARDS is complex and multifaceted involving 3 distinct components: (1) nature of the stimulus, (2) host response to the stimulus, and (3) the role of iatrogenic factors. To understand this complex process, it is important to understand the physiology and functional anatomy.
Physiology and functional anatomy
Human lung development begins with 50 million alveoli in the neonatal lung and completes with 500 million alveoli and approximately 50 m2 of surface area in an adult lung. A substantial part of alveolarization occurs during the first 2 years of life. The normal alveolar epithelium is comprised of two distinct types of cells. Type I alveolar cells are flat, account for 90% of the alveolar surface area and are covered with a thin layer of alveolar lining fluid. They participate in the gas exchange and are exposed to very high oxygen concentrations. Thus, they are vulnerable to oxidative injury, but recent literature suggests that type I cells may have an active system against the oxidative stress. They are end cells because they are incapable of proliferation and differentiation. They actually arise from type II cells. Type II alveolar cells are cuboidal or rounded cells that account for the remaining 10% of alveolar surface area and are resistant to injury. They do not participate in the gas exchange but are involved in surfactant production, ion transport, and other pulmonary defense mechanisms. [8, 9, 10, 11, 12, 13]
Alveolar epithelium and pulmonary microvascular endothelium create a two-layered alveolar-capillary barrier. This barrier serves the function of gas exchange, maintains the integrity of pulmonary morphology and protection from external injury. Disruption of this barrier results in increased permeability, influx of protein rich edema fluid into the alveolar sacs, dysfunction of surfactant production, and defective ion transport leading to impaired fluid clearance from alveolar cells. These changes are the hallmark of ARDS pathophysiology and are accompanied by dysregulated inflammation from dysfunctional leukocytes and influx of pro-inflammatory cytokines like interleukins and tumor-necrosis factor. The role of neutrophils in this mechanism is controversial. Animal models have favored both neutrophil dependent and neutrophil independent lung injury. It is also unclear if neutrophilic inflammation is the cause or the result of lung injury. Dysfunction of platelets and coagulation cascade results in microvascular thrombosis and capillary occlusion. [8, 9, 10, 11, 12, 13]
This course of ARDS pathophysiology was previously described in 3 histopathologic stages, including exudative, proliferative, and fibrotic phases. The timing of these stages is variable, and in fact, evidence suggests the beginning of resolution and fibrotic phase early in the course of ARDS. [11]
At the clinical level, respiratory distress occurs secondary to surfactant depletion, alveolar edema, cellular debris within the alveoli, and increased airway resistance. Surfactant loss leads to alveolar collapse because of increased surface tension, which is analogous to the situation observed in premature infants with infant respiratory distress syndrome (IRDS). As alveoli collapse, closing lung volume capacity rises above the patient’s functional residual capacity (FRC), further increasing atelectasis and the work of breathing. This is reflected as reduced lung. In addition, the remaining viable lung may be conceptualized as being smaller rather than stiff. Although the total lung compliance is reduced, a small portion of the lung may be participating in the gas exchange. Those remaining intact lung regions have better compliance and are thus subject to overdistention and potential air leak complications (eg, pneumothorax) when exposed to excessive inflating pressures.
The net effect is impairment in oxygenation. A widened interstitial space between the alveolus and the vascular endothelium decreases oxygen-diffusing capacity. Hypoxia arises as a result of the change described above. Collapsed alveoli result in either low ventilation-perfusion (V/Q) units or a right-to-left pulmonary shunt. The end result is marked venous admixture, the process whereby deoxygenated blood passing through the lungs does not absorb sufficient oxygen and causes a relative desaturation of arterial blood when it mixes with blood that is already oxygenated.
Pulmonary hypertension may also ensue from ARDS. Hypoxemia, hypercarbia, and small-vessel thrombosis together can elevate pulmonary arterial pressures. Persistent pulmonary hypertension can result in increased right ventricular work, right ventricular dilatation, and, ultimately, left ventricular outflow tract obstruction secondary to intraventricular septum shifting toward the left ventricle. These changes, in turn, may decrease cardiac output and further reduce oxygen delivery to vital organs.
Iatrogenic factors may further complicate the clinical picture. Oxygen toxicity, volutrauma, barotraumas, and fluid overload can further aggravate the lung injury and worsening lung compliance and oxygenation.
Resolution of ARDS is a very complex and active process. Alveolar edema resolves by active transport mechanism, where water follows sodium and chloride ions. Termination of inflammation involves anti-inflammatory mediators like IL-10, tissue growth factor (TGF) β and pre resolution mediators like polyunsaturated fatty acids, including lipoxins, resolvins, and protectins. Animal models have shown the role of platelets in repair of vascular endothelium, whereas epithelial repair is carried out by alveolar progenitor cells including type II alveolar cells, Clara cells and integrin α6β4 alveolar epithelial cells. [12] If the injury is severe, disorganized and insufficient, epithelial repair may result into fibrosis and loss of lung function.
The description of ARDS pathophysiology comes from adults and mature animal studies. Future research has been encouraged in pediatric populations and juvenile animals. [12]
Etiology
ARDS occurs as a consequence of diverse pulmonary and nonpulmonary etiologies. The most common conditions associated with ARDS are sepsis and infectious pneumonia (bacterial and viral). [9, 14, 15, 16, 17, 18] Sepsis-related ARDS cases may carry a poor prognosis if they are associated with shock and thrombocytopenia. [16] Other more common etiologies include bronchiolitis, aspiration pneumonia, aspiration of gastric contents, major trauma, pulmonary contusion, burns, inhalational injury, massive transfusions, or transfusion-related acute lung injury (TRALI). [9, 14, 15, 16, 17, 18] Transfusion of all types of blood products, including packed red blood cells, fresh frozen plasma, and platelets, has been associated with development of ARDS. [19, 20] Other causes include acute pancreatitis, fat embolism, envenomation, drowning or submersion injuries, drug reaction, malignancy, and lung transplantation. [9, 14, 15, 16, 17, 18] Ventilator-induced lung injury (VILI) has also been documented as one of the etiologies for development of ARDS. [21] Noninfectious lung injury can occur after stem cell transplantation. However, a separate entity of idiopathic pulmonary syndrome has been described as well in this context. [22, 23, 24]
Epidemiology
The incidence of ARDS is certainly lower in the pediatric population as compared to adults. The adult studies have reported a very wide range of incidence: from 17.9-86.2 per 100,000 person-years. [25, 26, 27, 28] For the population aged 15 years and older, age-adjusted incidence was 86.2 per 100,000 person-years, 38.5% hospital mortality; accounting for an estimated 190,600 cases of acute lung injury, 74,500 deaths, and 3.6 million hospital days each year in the United States. [28]
The incidence in the pediatric population is reported between 2.2 and 12.8 per 100,000 person-years. From the critical care perspective, ALI/ARDS accounts for 2.2% to 2.6% of pediatric intensive care unit (PICU) admissions, [14, 29] 8.3% of those receiving mechanical ventilation for more than 24 hours, [30] and PICU and hospital mortality ranging between 18% and 32.8%. [14, 31, 30, 32, 29]
The Pediatric Respiratory Distress Incidence and Epidemiology (PARDIE) study, which involved 27 countries, found that pediatric ARDS occurs in about 3% of patients in PICUs and in about 6% of those who are receiving mechanical ventilation. In addition, among mechanically ventilated patients, the greatest number of new cases of pediatric ARDS occurred in North America, in high-income countries, and during non-summer months. [33]
The age-related statistics of ARDS can be obtained by comparing the results of two different studies from King County, Washington, USA, that were conducted around the same time between 1999 and 2000. [28, 32]
Table. (Open Table in a new window)
Study |
Zimmerman JJ et al [32] |
Rubenfield GD et al [28] |
|
Age in years |
0.5 to 15 |
15 through 19 |
75 through 84 |
Incidence per 100,000 person-years |
12.8 |
16 |
306 |
Mortality |
18% |
24% |
60% |
Incidence and severity of ARDS are somewhat similar at different geographical locations. The study from Australia and New Zealand reported an incidence of 2.95 per 100,000 person-years, 2.2% of PICU admissions, and 30% of PICU mortality. [14] A Dutch study reported an incidence of 2.2 per 100,000 person-years and 20.4% mortality. [31] Investigators in Spain found an incidence of 3.9 per 100,000 patients-years and a PICU mortality of 26%. [30] A German study showed incidence of 3.2 per 100,000 person-years. [34] The incidence in the US-based study was a little higher at 12.8 per 100,000 person-years; however, mortality was slightly lower at 18%. [32] Search of the Chinese literature revealed 2.6% of PICU admissions were for ARDS, with a mortality of 32.8%. [29]
Of note, the above reported epidemiologic data are from studies prior to the Berlin definition, a study that eliminated the category of ALI and classified ARDS as mild, moderate, and severe. Thus, the epidemiology of both ALI and ARDS has been included here.
Environmental and genetic influences
ARDS develops after the insult from diverse etiologies discussed above. However, the heterogeneity of susceptibility and outcomes is intriguing. This could partially be explained by environmental and genetic influences. Research is still growing in this area.
From an environmental standpoint, literature from adult populations has shown increased risk of ARDS with alcohol abuse [35, 36] and smoking (active and passive) after blunt trauma. [37] The association of passive smoking could be applied to the pediatric population.
From a genetic standpoint, a total of 34 genes have been reported to impact ARDS susceptibility. [38] The majority of them are linked to the currently described pathophysiological pathways of ARDS. These include inflammation, epithelial cell function, endothelial cell function, coagulation, oxidative injuries, apoptosis, and platelet cellular process. [38, 39, 40] [41, 42] The other reported genetic mutations associated with ARDS were linked to surfactant dysfunction [38] and to the epidermal growth factor gene polymorphism in males. [43]
There is not enough literature suggesting ethnic differences for ARDS incidence and outcomes. The vast majority of initial genetic studies were in European populations. The literature is scant for other ethnic backgrounds. Thus far, approximately nine genes in African population and three genes in Asian population have been reported to be linked with ARDS. [38] Studies have reported poor outcomes in African Americans with ARDS as compared to patients of other ethnicities. [44, 45, 46] However, in one study, higher mortality was associated with greater severity of illness on presentation in Black patients. Higher mortality in Hispanic patients was not explainable by severity of illness on presentation in the same study. [45]
Some of the epidemiologic studies have reported a slightly higher incidence of ARDS among male children (54-63%) [14, 30, 32] ; however, the mortality (31% in male children) was not significantly different. [14] One adult study reported higher mortality among males. [46]
There is also not enough literature in the area of genetics pertinent to pediatric ARDS in the context of growing lungs and developing immunity. [2]
Prognosis
Complications
Several complications are associated with ARDS, though many of these are due to the precipitating conditions that lead to ARDS. Acute complications include air-leak syndromes, ventilator-induced lung infection (VILI), and multiple organ dysfunction syndrome (MODS), although definitive evidence linking this syndrome to ARDS or ventilator use remains controversial.
Numerous pulmonary complications may result from ARDS. The most common are the air-leak syndromes, particularly pneumothorax but also pneumomediastinum, pneumopericardium, pneumoperitoneum, and subcutaneous emphysema. Features of a pneumothorax include decreased air entry on the side of the air leak, an increased percussion note on the same side, and tracheal deviation away from the affected side in a tension pneumothorax. Heart sounds may be muffled, and signs of decreased cardiac output may be observed with a tension pneumothorax. Clinicians must also maintain a high index of suspicion for tension pneumothoraces as a cause for acute onset of decreased cardiac output.
VILI is an entity receiving attention with the publication of landmark trials suggesting that a “kinder, gentler” form of mechanical ventilation improves outcomes in ARDS. VILI most likely has several causes, including excessive lung stretching due to high tidal volumes, repetitive opening and closing of alveoli leading to shear stress, oxygen toxicity, and cytokine release.
ARDS patients may also be compromised from a cardiovascular standpoint. Patients with sepsis, trauma, or other multisystem insults may lose their ability to tolerate higher airway pressures often required to maintain adequate oxygenation. Higher airway pressures lead to a higher net intrathoracic pressure, which results in decreased preload and cardiac output. Moreover, hypoxia, hypercarbia, and acidosis may elevate pulmonary artery pressures, increasing right ventricular afterload and leading to increased right ventricular work. Right ventricular dilatation can develop and then result in leftward movement of the intraventricular septum and cause left ventricular outflow tract obstruction.
Gastrointestinal complications commonly observed in the critically ill population include stress ulcers, liver failure, pancreatitis, and pancreatic insufficiency, leading to glucose intolerance.
Renal failure may result from the primary illness or may occur secondarily as a result of poor cardiac output, acute tubular necrosis, and MODS.
Secondary or nosocomial pneumonia is not uncommon in critically ill children. In addition to Staphylococcus aureus, other organisms more typically isolated include Pseudomonas species, Acinetobacter baumannii, Stenotrophomonas maltophilia, Escherichia coli, and Candida species. Bacteremia from indwelling vascular catheters and skin ulcerations may also occur. Risk of urinary tract infection increases with prolonged indwelling Foley catheters.
Critical illness polyneuropathy and myopathy (CIPNM) is seen in a subset of patients of unclear etiology. Many factors have been identified to have an increased association with CIPNM, such as sepsis, systemic inflammatory response syndrome, MODS, and prolonged mechanical ventilation. Use of muscle relaxants, especially in conjunction with steroids, appears to have a particularly high association with CIPNM. Initial reports describe CIPNM with concomitant use of nondepolarizing muscle relaxants and corticosteroids. However, case reports of weakness with cisatracurium and corticosteroids have also been described. Clinically, patients develop profound or flaccid weakness that is often prolonged. This may complicate the mechanical ventilator weaning process and may also require inpatient rehabilitation care upon discharge from the hospital. [47, 48]
-
Eight-year-old girl with diagnosis of pneumonia. Chest radiograph on day of admission.
-
Fourteen-month-old boy with diagnosis of exacerbation of bronchopulmonary dysplasia. Chest radiograph on day of admission.
-
Eight-year-old girl with pneumonia and impending respiratory failure. Chest radiograph on day 2.
-
Fourteen-month-old boy with exacerbation of bronchopulmonary dysplasia and impending respiratory failure. Chest radiograph on morning of day 2.
-
Fourteen-month-old boy with exacerbation of bronchopulmonary dysplasia and respiratory failure. Chest radiograph on afternoon of day 2.
-
Fourteen-month-old boy with exacerbation of bronchopulmonary dysplasia, respiratory failure, and severe hypoxemia. Chest radiograph on evening of day 2.
-
Chest radiograph in 3-year-old girl who developed acute respiratory distress syndrome due to overwhelming gram-negative sepsis. Salient features include endotracheal tube; diffuse, bilateral infiltrates; air bronchograms on left side; and central venous catheter. Ratio of arterial oxygen tension to fraction of inspired oxygen at time of chest radiography was 100.
-
Chest radiograph demonstrates complication of acute respiratory distress syndrome. Patient presented with respiratory failure after near-drowning episode. Peak inspiratory pressures were 40 cm water. Patient had sudden desaturation and decreased bilateral air entry, as well as cool peripheries and decreased blood pressure. Needle evacuation of both pleural spaces confirmed pleural air. Chest tubes were placed, with immediate improvement in clinical status. Pulmonary status continued to deteriorate; high-frequency oscillatory ventilation was given. Patient subsequently required second chest tube on left side.
-
Chest CT in 6-month-old male infant with newly diagnosed cystic fibrosis. Patient was intubated for respiratory failure and subsequently developed acute respiratory distress syndrome. Image demonstrates numerous cystic and bronchiectatic areas. Note dorsal distribution of atelectasis, particularly on right side.
-
Typical pressure-volume curve may provide information regarding lung compliance, lung hysteresis, and critical opening and closing pressures. Evidence of pulmonary overdistention may also be observed.
-
Subcutaneous emphysema and pneumothorax.
Tables
| FiO2 | 0.3 | 0.4 | 0.5 | 0.6 | 0.7 | 0.8 | 0.9 | 1 |
|---|---|---|---|---|---|---|---|---|
| PEEP | 5 | 6-8 | 8-10 | 10 | 10-14 | 14 | 14-18 | 18-24 |







