Practice Essentials
Chest pain is a common reason parents seek medical attention for their children. Annually, physicians evaluate >600,000 cases of chest pain in patients aged 10-21 years, a number that may reflect overwhelming concern about chest pain as a manifestation of cardiac disease as noted in older patients. [1, 2]
Costochondritis is a common cause of chest pain in children and adolescents. The condition is characterized as an inflammatory process of one or more of the costochondral cartilages that causes localized tenderness and pain of the anterior chest wall. [3, 4] (See the image below.) Most cases of costochondritis are idiopathic. The remaining cases may result from costochondral irritation due to direct trauma to the area, aggressive exercise resulting in a strain of the costochondral cartilage, or a prior upper respiratory tract infection with cough which can cause repeated stretching and strain at the costochondral junction resulting in local irritation and pain.
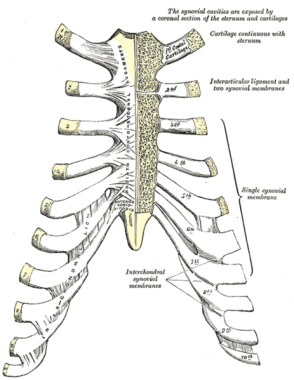 Sternocostal and interchondral articulations. Anterior view.
Sternocostal and interchondral articulations. Anterior view.
Costochondritis is a relatively benign and usually self-limited condition, although symptoms can persist for up to 3 months. [5] Patients are often evaluated initially in the emergency department (ED) or in their primary care physician's office.
The term Tietze syndrome implies swelling; costochondritis refers to pain alone.
Pathophysiology
The exact pathophysiology of cartilage and capsular involvement is unknown because costochondritis does not warrant surgical intervention or tissue biopsy. Theoretically, the cartilage involved in costochondritis is either inflamed or fractured. Either condition presumably leads to inflammation with subsequent stimulation of pain receptors.
Etiology
Most cases of costochondritis are idiopathic. The remaining cases may be the result of costochondral irritation caused by the following:
-
Direct trauma
-
Aggressive exercise resulting in a strain (eg, repeated twisting of the upper torso, stretching-pulling activities of the upper extremities) [6]
-
Preceding upper respiratory tract infection with cough (which can cause repeated stretching and strain at the costochondral junction)
Collins et al reported the case of an 11-year-old boy with severe costochondritis following coronavirus disease 2019 (COVID-19) infection. [7]
Epidemiology
United States statistics
Several studies of chest pain in pediatric patients report costochondritis prevalences of 14-32%. [5, 1, 8, 9] A single study reported rates as high as 79% [10] ; however, this higher prevalence may be due to less stringent diagnostic criteria for costochondritis. The overall incidence is approximately 4% in children and adolescents.
Race-, sex-, and age-related demographics
Race
A study indicates Hispanics may have an increased prevalence of costochondritis, but most studies do not mention race as a factor. [11]
Sex
Studies of chest pain in children demonstrate that males and females are affected equally. There are no recent studies evaluating the effect of gender in costochondritis.
Age
No data support an association between age and costochondritis; the condition is well described in children of all ages, including infants. [12]
Prognosis
The overall prognosis of a patient with costochondritis is excellent and full recovery can be expected.
Driscoll described the average length of symptoms for costochondritis as 96 days in duration, so while prognosis is excellent, recovery can be somewhat prolonged. [5]
Resolution rarely lasts longer than 4-6 months. Relapse may occur if the patient returns to activity while still symptomatic.
Morbidity/mortality
No reports have associated mortality with costochondritis, and no mortality is expected.
-
Sternocostal and interchondral articulations. Anterior view.

