Practice Essentials
The need for vascular access in the pediatric patient is frequent [1] ; however, placement of a peripheral line may not be feasible or appropriate. The options available to clinicians have increased over the years; central venous access devices (CVADs) are now used with greater frequency. This article discusses the various options available for central venous access and their advantages, disadvantages, and complications.
CVADs include peripherally inserted central catheters (PICCs), central venous catheters (CVCs), implantable access ports (IAPs), umbilical artery catheters (UACs), and umbilical vein catheters (UVCs). CVADs can be placed in numerous sites, including the internal jugular vein (IJV), the subclavian vein, the femoral vein, peripheral veins leading to central access, and other surgical access sites. (See Treatment, Approach Considerations.)
Advances in equipment have made the use of CVADs safer and more common. CVADs come in many different sizes and brands that allow the clinician to choose the best device for each patient. However, the small sizes of the devices and of pediatric patients can complicate CVAD procedures in children. [2]
Future research is likely to focus on the material used in CVADs, as well as on means of preventing infection and occlusion. Ultrasonography (US) has become a useful adjunct in the placement of central lines. [3, 4, 5, 6] Pediatric and emergency medicine training programs will benefit from teaching and using US for central line placements. [7] Increasing attention is being paid to preserving central access in children with chronic illness, who often require prolonged or repeated venous access and who are at high risk for venous catheter–related complications that largely derive from elective decisions during catheter insertion and continuing care. [8, 9]
Anatomy
After the decision has been made to place a CVAD, a suitable approach is chosen. A clear understanding of the anatomy is needed for each of the different approaches. The four main approaches to central venous access discussed here include the internal jugular, subclavian, femoral, and PICC techniques.
Internal jugular approach
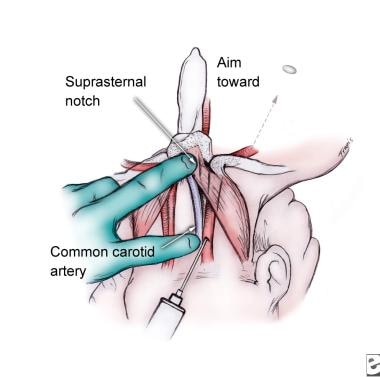
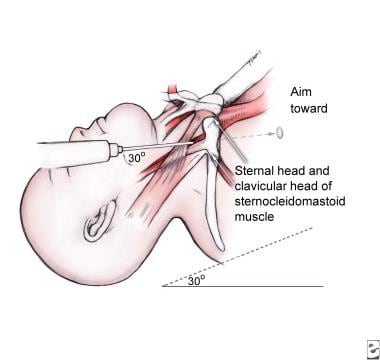
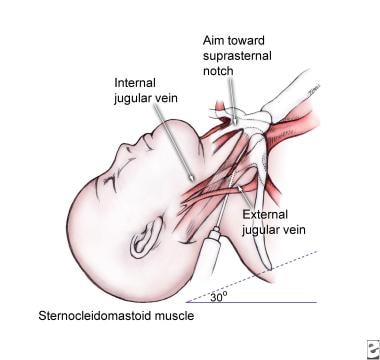
The IJV lies parallel and lateral to the carotid artery in the neck. (See the images below.) It lies within the carotid sheath, which includes the carotid artery and vagus nerve. The IJV is a branch of the brachiocephalic vein.
Subclavian approach
The subclavian artery lies posterior and somewhat superior to the brachiocephalic vein. These two vessels are separated by the anterior scalene muscles. The subclavian vein begins distal to the branch point of the IJV. It crosses under the clavicle at the medial to proximal third of the clavicle. The subclavian artery is located deep and slightly superior to the vein.
In children, the subclavian vein has a more cephalic location than it does in adults; it dives under the clavicle closer to the medial third.
Deep to the vessels lies the first rib, which is just superficial to the pleura and lung.
Femoral approach
The femoral vein is a branch of the external iliac vein. (See the image below.) It crosses deep to the medial third of the inguinal ligament. A common mnemonic for the anatomy of the femoral vessels from lateral to medial is NAVEL (Nerve, Artery, Vein, Empty space, Lymphatics).
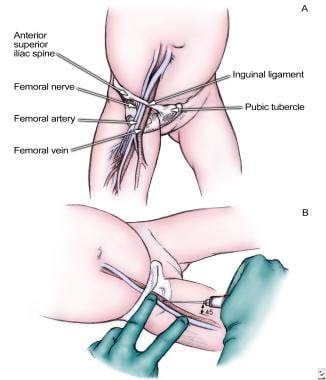 Femoral vein approach. Remember mnemonic NAVEL: nerve, artery, vein, empty space, and lymphatics.
Femoral vein approach. Remember mnemonic NAVEL: nerve, artery, vein, empty space, and lymphatics.
Peripherally inserted central catheter approach
The relevant anatomy for inserting a PICC line includes the superficial veins to be used. These are primarily located in the arms (cephalic and basilic veins), scalp (superficial temporal vein), or neck (external jugular vein [10] [EJV]).
The umbilical system consists of two arteries and one vein (see the image below). The vein is usually at the 12-o'clock position and is larger with thinner walls, whereas the arteries are located inferiorly with thicker walls. Occasionally, a persistent urachus may be encountered and mistaken for the vein; however, a return of urine quickly reveals the error.

The vein travels to the inferior vena cava (IVC), or it could turn to the portal system. The umbilical artery turns inferiorly and then continues to the pelvis, where it meets the internal iliac artery continuing cephalad to the bifurcation of the aorta.
Epidemiology
Approximately 5 million CVC insertions are performed every year in the United States. This rate accounts for 15 million CVC days each year in the intensive care unit (ICU). The use of CVCs in the ICU is similar in adult and pediatric patients.
Prognosis
The outcome and prognosis of patients with a CVAD directly depend on the complications (see Treatment, Complications). If complications are minimized, the outcome related to placement of these lines is excellent. In addition, meticulous and sterile care of the CVAD can help prevent line infections.
-
Femoral vein approach. Remember mnemonic NAVEL: nerve, artery, vein, empty space, and lymphatics.
-
Umbilical vein cannulation in newborn.
-
Internal jugular vein, anterior approach.
-
Subclavian vein approach.
-
Internal jugular vein, central approach.
-
Internal jugular vein, posterior approach.
Tables
Age (y) |
Weight (kg) |
Gauge |
French |
Length (cm) |
< 1, newborn |
4-8 |
24 |
3.0 |
5-12 |
< 1 |
5-10 |
22 |
3.0-3.5 |
5-12 |
1-3 |
10-15 |
20 |
4.0 |
5-15 |
3-8 |
15-30 |
18-20 |
4.0-5.0 |
5-25 |
>8 |
30-70 |
16-20 |
5.0-8.0 |
5-30 |







