Practice Essentials
Pediatric sepsis is generally considered to comprise a spectrum of disorders that result from infection by bacteria, viruses, fungi, or parasites or the toxic products of these microorganisms. Early recognition and intervention clearly improve outcome for infants and children with conditions that lead to sepsis.
The spectrum of sepsis ranges from microbial invasion of the bloodstream or intoxication with early signs of circulatory compromise—including tachycardia, tachypnea, peripheral vasodilation, and fever (or hypothermia)—to full-blown circulatory collapse with multiple organ dysfunction syndrome (MODS) and death (see the image below).
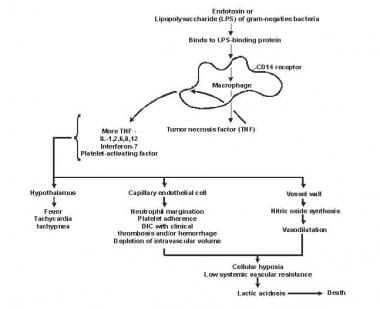 Pathogenesis of sepsis and multiple organ dysfunction syndrome (MODS).
Pathogenesis of sepsis and multiple organ dysfunction syndrome (MODS).
Signs and symptoms
Obtain a complete history as part of the evaluation for possible sepsis. Symptoms that may be noted include the following:
-
Fever (most common presenting symptom of children with systemic inflammatory response syndrome [SIRS])
-
Racing heart
-
Rapid or labored breathing
-
Cool extremities
-
Color changes
The following should be inquired into:
-
Exposures to infectious illnesses and other sources of insult
-
Activity level
-
Mental status (relative to age)
-
Urine output
-
Immunizations
-
Drug allergies
Perform a complete physical examination. Findings reflective of sepsis may include the following:
-
Subtle changes in vital signs (often the first indicators of impending SIRS)
-
Hypotension, mental status changes, and anuria (late signs)
-
Hypothermia (often more ominous than fever)
-
Localizing signs of infection
See Presentation for more detail.
Diagnosis
Laboratory studies that may be helpful include the following:
-
Complete blood count (CBC)
-
Measures of clotting function and coagulation parameters.
-
Electrolyte levels
-
Renal and liver function tests
-
Etiology-specific serologies
-
Urinalysis
-
Tests for inflammatory markers and acute-phase reactants
-
Culture of blood, urine, cerebrospinal fluid (CSF), or other tissues
Other studies that may be considered, depending on the clinical context, are as follows:
-
Chest radiography
-
Computed tomography (CT)
-
Magnetic resonance imaging [MRI)
-
Echocardiography.
-
Lumbar puncture for CSF evaluation
See Workup for more detail.
Management
The initial focus of treatment is on stabilization and correction of metabolic, circulatory, and respiratory abnormalities, which may include the following:
-
Aggressive fluid resuscitation and support of cardiac output
-
Ventilatory support with supplemental oxygen therapy
-
Maintenance of adequate hemoglobin concentration
-
Correction of physiologic and metabolic derangements
-
Monitoring of urine output and other end-organ functioning
Antimicrobial agents should be given as soon as possible, according to the most likely pathogens. The following therapies are commonly employed:
-
Newborns and infants in the first 6-8 weeks of life: Ampicillin and gentamicin, ampicillin and cefotaxime, or ampicillin and ceftriaxone
-
Older infants and children with sepsis of unclear etiology: A third-generation cephalosporin plus vancomycin. Add clindamycin if S aureus or GABHS are possible etiologies.
-
Patients who have indwelling catheters or those who are at high risk for methicillin-resistant Staphylococcus aureus (MRSA) infection: As above, with the addition of vancomycin
-
Patients who have fever and neutropenia: Broad-spectrum coverage with an emphasis on Gram-negative rods
Surgical intervention (eg, abscess drainage or venous access) is occasionally required.
Adjunctive therapies may be considered, including the following:
-
Inhaled nitric oxide
-
Extracorporeal membrane oxygenation
-
Corticosteroids
-
Pentoxifylline
-
Intravenous immunoglobulin (IVIg)
-
Terlipressin
-
Bovine lactoferrin
Generally, these patients should not be fed until gut hypoxia and hypoperfusion have been excluded. Once feeding can safely begin, immune-enhancing nutrition may reduce mortality.
See Treatment and Medication for more detail.
Background
Pediatric sepsis, like sepsis in adults, is generally considered to comprise a spectrum of disorders that result from infection by bacteria, viruses, fungi, or parasites or the toxic products of these microorganisms. (See also Neonatal Sepsis.) The terms bacteremia, viremia, fungemia, and parasitemia refer to bloodstream invasions (BSIs) that may be associated with fever but have no other signs or symptoms of circulatory compromise or end-organ malperfusion or dysfunction.
Sepsis is a problem that presents a management challenge to those who care for infants and children; however, early recognition and intervention clearly improves the outcome for infants and children with infections or intoxications that lead to sepsis.
Most infants and children with sepsis require monitoring and treatment in an intensive care setting. Initial focus should be on stabilization and correction of metabolic, circulatory, and respiratory derangements. Appropriate antimicrobial therapy should be started as soon as possible after evaluation occurs. Ongoing reevaluation is essential.
Critical care expertise is essential for moderate-to-severe cases. Consultation with an infectious diseases specialist may be necessary. Other consultations should be obtained in accordance with the specific clinical circumstances.
A report on sepsis by the CDC that included a retrospective review of 246 adult and 79 pediatric patients (31 infants younger than 1 year and 48 children between 1 and 17 years of age) with severe sepsis or septic shock found that nearly 80% of patients develop infections leading to sepsis outside a hospital. The study also found that 7 in 10 sepsis patients had seen a healthcare provider in the month preceding sepsis admission or had chronic diseases requiring frequent medical care. [1, 2]
Pathophysiology
The spectrum of sepsis ranges from microbial invasion of the bloodstream or intoxication with early signs of circulatory compromise—including tachycardia, tachypnea, peripheral vasodilation, and fever (or hypothermia)—to full-blown circulatory collapse with multiple organ dysfunction syndrome (MODS) and death (see the image below).
Pathogenesis of sepsis and multiple organ dysfunction syndrome (MODS).
All these manifestations are part of what is more appropriately termed the systemic inflammatory response syndrome (SIRS), which may be caused by noninfectious or infectious conditions. SIRS results from an insult (infectious, traumatic, chemical, malignant, autoimmune, or idiopathic) and the host response to the insult. The outcome depends on the intricate interplay of upregulating and downregulating cytokines and inflammatory cells and the direct effects of the insult itself. Sepsis is SIRS developing in conjunction with infection.
Experts have come together to develop a consensus on definitions of sepsis, SIRS, severe sepsis, and septic shock that are appropriate for the pediatric population. [3] Age-related variables have been applied to the definition of SIRS and sepsis. The definition of SIRS now requires either fever or white blood cell (WBC) abnormality.
The earliest, mildest manifestation of SIRS is typified by the triad of hyperthermia (or hypothermia), tachypnea, and tachycardia. If SIRS is identified and reversed early, the subsequent inflammatory cascade can often be avoided or mitigated. However, in some situations, further damage occurs because the insult or the resultant host immune response is too great. This damage can result in increased cardiac output, peripheral vasodilation, increased tissue oxygen consumption, and a hypermetabolic state (ie, warm shock).
If SIRS is not identified and reversed early, cardiac output may fall, peripheral vascular resistance may increase, and shunting of blood may ensue (ie, cold shock). This results in tissue hypoxia, end-organ dysfunction, metabolic acidosis, end-organ injury or failure, and death.
Etiology
Bacterial causes
Myriad bacteria, viruses, fungi, and parasites can cause sepsis. Among the bacterial causes of sepsis, the following age-related patterns are observed. [4]
In patients with early-onset neonatal sepsis, Streptococcus agalactiae, Escherichia coli, Haemophilus influenzae, and Listeria monocytogenes are the most frequent organisms encountered.
In patients with late-onset neonatal sepsis, coagulase-negative Staphylococcus, [5] Staphylococcus aureus, E coli, Klebsiella species, Pseudomonas aeruginosa, Enterobacter species, Candida species, S agalactiae, Serratia species, Acinetobacter species, and various anaerobes are some of the most commonly involved organisms.
In most infants worldwide, the most frequent causes of bacterial sepsis are H influenzae type b (Hib), Streptococcus pneumoniae, Neisseria meningitidis, and Salmonella species. In the United States and the developed world, E coli, S aureus, S pneumoniae, and Nmeningitidis predominate because conjugate Hib vaccination has essentially eliminated disease caused by Hib and conjugate pneumococcal vaccination has significantly decreased the incidence of that infection. [6] In regions where malaria occurs, Plasmodium falciparum is a frequent cause of SIRS in infancy.
The same pathogens that cause sepsis in infancy also cause it in childhood, although the presence of encapsulated organisms generally becomes less frequent as a child’s immune response to polysaccharide antigens improves with age.
Risk factors
Underlying conditions predispose to infection with particular pathogens, such as the following:
-
AIDS predisposes to sepsis from various usual and unusual pathogens, particularly pneumococcus
-
Children with hemoglobin SS disease have a 400-fold increased risk of sepsis due to pneumococcus and Salmonella, among other pathogens
-
Congenital heart disease is a risk factor for endocarditis and sepsis, and genitourinary anomalies often increase the risk of urosepsis
-
Infants and children with significant burns are at risk for sepsis caused by skin flora and nosocomial gram-negative pathogens in particular
-
Splenic dysfunction or absence, as well as complement, immunoglobulin, and properdin deficiency, predispose to sepsis due to encapsulated organisms
-
Infants and children with hematologic and solid-organ malignancies (before or during treatment) are at increased risk for sepsis from a considerable variety of organisms
-
Neonates, infants, and children who are hospitalized (particularly in the intensive care unit [ICU]) are at increased risk for SIRS
-
Those with indwelling devices or prosthetic material and other breaches in barrier protective function are also at increased risk for SIRS
In a retrospective cohort study of 3967 infants in the neonatal intensive care unit who underwent placement of 4797 peripherally inserted central catheters (PICCs), Milstone et al found that the risk of central-line-associated bloodstream infection (CLABSI) increased steadily in the initial 2 weeks following catheter insertion and remained high thereafter. After adjustment for independent predictors of CLABSI, the risk was higher in infants with a catheter dwell time of more than 2 weeks than in infants with a shorter dwell time. [7, 8]
Epidemiology
SIRS remains an infrequent but significant cause of death among infants and children in the United States. The incidence of sepsis is somewhat higher in the developing world than it is in the United States. However, reports are fewer, and precise figures are unavailable.
The risk of sepsis is inversely related to age. Neonates are at the highest risk, with bacterial sepsis occurring in 1-10 per 1000 live births in the United States. No sex predilection for sepsis is known, except for urosepsis, which is more common in females and uncircumcised males. No particular racial predilection is noted for sepsis, except that invasive bacterial infections are more common in Eskimos, American Indians, and individuals with hemoglobin SS disease.
A review of 20-year trends in maternal/neonatal care, complications, and mortality among extremely preterm infants born at Neonatal Research Network centers reported that despite no improvement from 1993 to 2004, rates of late-onset sepsis declined between 2005 and 2012 for infants of each gestational age. [9]
McMullan et al conducted a study to describe the epidemiology of Staphylococcus aureus bacteremia in children and adolescents younger than 18 years from Australia and New Zealand. The study found that of the 1073 children with SAB who had complete outcome data available, the median age was 57 months, and that the annual incidence for Australian children was 8.3 per 100 000 population and was higher in indigenous children. The study also found that seven- and 30-day mortality rates were 2.6% and 4.7%, respectively and risk factors for mortality were age younger than 1 year; Māori or Pacific ethnicity; endocarditis, pneumonia, or sepsis; and receiving no treatment or treatment with vancomycin. [10]
Prognosis
Mortality from pediatric sepsis ranges from 9% to 35%. Different insults are associated with different outcomes. Host immune status is important in determining outcome. Aggressive fluid resuscitation early in the course of SIRS results in decreased mortality (except, possibly, in resource-limited, developing countries). [11, 12]
Almost half of neonatal deaths are caused by sepsis, although advances in diagnosis and treatment have caused this rate to decrease substantially, especially in preterm infants. Again, mortality tends to decrease as age increases in the pediatric population.
A US study that included 9816 children with severe sepsis found that mortality was significantly higher in Black children (18.4%) than in White (13.4%) or Hispanic children (13.7%). Overall, Black children had a greater odds of dying of sepsis than did White children (adjusted odds ratio, 1.19). [13]
Patient Education
Parents of newborns should understand that any fever in the first few months of life necessitates immediate evaluation. The importance of fever as a marker of possible serious infection, rather than a concerning symptom itself, should be emphasized.
Front-line providers must recognize the importance of aggressive resuscitation for the patient with early signs of SIRS.
Vaccination is the key to preventing many of these infections. Travelers should be warned of the possibility of serious infections during travel.
For patient education information, see the Infections Center, as well as Sepsis.
-
Pathogenesis of sepsis and multiple organ dysfunction syndrome (MODS).