Practice Essentials
Human metapneumovirus (hMPV) is a respiratory viral pathogen that causes a spectrum of illnesses that range from asymptomatic infection to severe bronchiolitis. In 2001, van den Hoogen et al described the identification of this new human viral pathogen from respiratory samples submitted for viral culture during the winter season. [1] Half of the initial 28 human metapneumovirus isolates were cultured from patients younger than 1 year, and 96% were isolated from children younger than 6 years.
Seroprevalence studies revealed that 25% of all children aged 6-12 months who were tested in the Netherlands had detectable antibodies to human metapneumovirus; by age 5 years, 100% of patients showed evidence of past infection. Separate reports from all areas of the world support the early contention that this newly discovered virus is ubiquitous, and, like human respiratory syncytial virus (RSV) infection, is seasonal in nature. [2]
Although the description of this viral pathogen was first described in children, subsequent reports have highlighted the importance of human metapneumovirus as a cause of respiratory illness in adults of all ages, [3, 4] in patients with cancer, [5] in the elderly population (as a cause of serious lower respiratory tract infection), [6] and in adults with underlying chronic medical conditions. [7]
Pathophysiology
The pathophysiology of human metapneumovirus infection is thought to be closely related to the other common human pneumovirus, RSV. Like RSV, human metapneumovirus has a tropism for the respiratory epithelium. The patient may be asymptomatic, or symptoms may range from mild upper respiratory tract symptoms to severe bronchiolitis and pneumonia. More than 20% of infants with bronchiolitis have been found to be infected with two or more respiratory pathogens at the same time. Of these, more than 10% have been described to be co-infected with human metapneumovirus. [8, 9] Viremia from human metapneumovirus infection has not yet been demonstrated, but a 2005 reported case of human metapneumovirus encephalitis with concurrent lung disease supports the possibility that the virus may (rarely) enter the bloodstream.
Etiology
The respiratory viral pathogen human metapneumovirus causes a spectrum of illnesses, which range from asymptomatic infection to severe bronchiolitis. Human respiratory syncytial virus (RSV), parainfluenza virus type 1, human metapneumovirus, and human parainfluenza virus type 3 are all known to cause clinical bronchiolitis. Although RSV has been reported to cause as many as 90% of bronchiolitis cases in infants, the relative contribution of human metapneumovirus remains undetermined.
Human metapneumovirus is a negative-sense nonsegmented RNA virus that has been categorized in the pneumovirus subfamily, family Paramyxoviridae, based on genomic sequence and gene constellation.
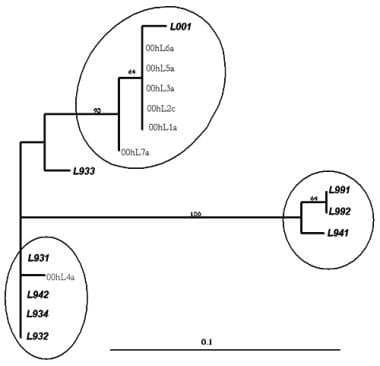 Phylogenetic tree showing sequence analysis of human metapneumovirus (HMPV).
Phylogenetic tree showing sequence analysis of human metapneumovirus (HMPV).
Epidemiology
United States statistics
Human metapneumovirus infection is very common. Estimates suggest that this virus is the causative agent of infant bronchiolitis in 5-15% of cases. Children infected with respiratory viruses, such as human metapneumovirus, are frequently co-infected with other common respiratory viruses. [8, 9]
International statistics
Seroprevalence studies revealed that 25% of all children aged 6-12 months who were tested in the Netherlands had detectable antibodies to human metapneumovirus; by age 5 years, 100% of patients showed evidence of past infection. In Australia, 3 of 200 (1.5%) randomly chosen respiratory samples with negative results for the presence of known respiratory pathogens had positive results for human metapneumovirus on culture, polymerase chain reaction, or both.
Race-, sex-, and age-related demographics
To date, no racial predilection has been described.
Females accounted for 31% of the patients originally described to have human metapneumovirus infection.
Human metapneumovirus infection is prevalent during infancy and early childhood. [10] By age 5 years, seroprevalence data suggest infection in all (or nearly all) individuals. Available demographic data are limited to the Netherlands, where the virus was originally identified in 2001. Further epidemiologic investigation is needed to determine prevalence in other areas of the world. The role of human metapneumovirus in causing respiratory illness in adults has been explored in detail, highlighting the potential severity of human metapneumovirus infection in elderly patients, [6] including outbreaks of severe illness among elderly persons in long-term care facilities. [11]
Prognosis
The prognosis appears excellent, but further information is needed.
Complications
Respiratory failure may develop.
-
Phylogenetic tree showing sequence analysis of human metapneumovirus (HMPV).






