Practice Essentials
Burn care should begin at the site of injury and continue through prehospital care and transportation to the closest burn center, or to the closest emergency department (ED) with advanced life support capability, followed by transfer to a burn center when appropriate.
The image below depicts partial- and full-thickness burns.
 Partial- and full-thickness burns from a structure fire. Note facial involvement.
Partial- and full-thickness burns from a structure fire. Note facial involvement.
See Thermal Injuries: A Matter of Degree, a Critical Images slideshow, to help identify and treat various types and degrees of burn injuries.
Prehospital care
Remove the person from the source of the burn without endangering rescue personnel. After extrication, initial care of the burn victim should follow the basic principles of trauma resuscitation (ie, airway, breathing, and circulation [ABCs]), as follows:
-
Perform a rapid primary survey and immediately correct any problems found
-
Remove any constricting clothing and jewelry
-
When ventilatory and circulatory competence have been restored, perform a secondary survey
-
Concurrently with airway and circulatory management, make an effort to stop the burning process
Airway and breathing support
-
Administer humidified oxygen via a nonrebreathing reservoir mask or endotracheal tube at a rate of 10-12 L/min if signs of inhalation injury are present
-
A patient who is not breathing should be intubated and ventilated with 100% oxygen
Treatment of burn shock
-
Administer humidified oxygen
-
Administer IV fluids if transport time will be longer than 30 min and fluid resuscitation is indicated
Fluid resuscitation
-
Begin resuscitation immediately with warmed fluids if possible
-
The arm is the preferred site for cannulation
-
Catheters may be placed through burned skin if unburned skin is unavailable
-
If IV access is not possible, consider interosseous access methods
-
Fluid resuscitation is not recommended for children at the scene of the accident
-
In adults, administer lactated Ringer solution or normal saline without glucose
-
IV flow rates are determined according to the patient’s clinical status
Cooling of burned tissue
-
Remove charred clothing
-
Immerse the burn wound in cold (1-5°C) water for about 30 minutes if transport cannot be undertaken immediately
-
Do not use ice water or apply ice directly to the burn wound
-
Local cooling of burns of less than 9% of TBSA can be continued longer than 30 min to relieve pain
-
Minor burns can be cooled with running tap water and dressed after more life-threatening issues have been addressed
Transfer to burn center
-
If the vehicle with advanced life support capability can transport the burn patient to a specialized burn treatment facility within 30 minutes, the patient should be taken directly to this facility
-
If the transport time to the specialized burn treatment facility is longer than 30 minutes, the patient should be transported instead to the nearest ED with advanced life support capability
Initial emergency department treatment
When the patient arrives in the ED, treatment is as follows:
-
Perform a rapid initial assessment of respiratory and cardiovascular status
-
Establish the extent and depth of burn injury
-
Determine the need for special procedures
-
Cool minor burns with towels moistened with cool sterile saline
-
Debride any open blisters
-
Fingers and toes should be wrapped individually, with fluffed gauze separating the digits
-
Cover all partial-thickness wounds with antibiotic ointment
-
Cleanse other areas with minor burns with the use of a mild soap and gentle scrubbing
-
Check tetanus status of all patients and administer tetanus immunization as appropriate
-
Discharge the patient with explicit wound care instructions and arrange follow-up for wound evaluation
Airway and respiratory care
-
Early intubation rather than observation is recommended in patients with signs of upper airway injury
-
Fiberoptic bronchoscopy helps in diagnosing acute inhalation injury, intubating patients with inhalation injury, and administering supplementary oxygen
-
With full-thickness burns of the neck, a vertical incision through the eschar extending from the sternal notch to the chin helps maintain a patent airway
-
If respiratory insufficiency is caused by a constricting eschar of the anterior thorax that limits respiratory excursion, escharotomy is imperative
-
If respiratory failure ensues, mechanical ventilation is necessary
-
Ventilator settings may have to be adjusted to slightly higher respiratory rates (16-20 breaths/min) and smaller tidal volumes (7-8 mL/kg)
-
High-frequency flow-interruption ventilation appears useful
-
Oscillating ventilator may be preferred after smoke injury
-
For elevated carboxyhemoglobin (COHb) levels, give 100% oxygen until the COHb level is below 10%; patients who have elevated COHb levels and a pH < 7.4 should be treated with hyperbaric oxygenation
-
Consider empiric treatment for cyanide toxicity for patients with unexplained severe metabolic acidosis, elevated central venous oxygen content, normal arterial oxygen content, and a low COHb level
Fluid resuscitation
-
Place 1 or 2 large-bore peripheral lines and administer crystalloids (eg, lactated Ringer solution)
-
Patients with burn wounds smaller than 20% of total body surface area (TBSA) can be treated with a combination of oral and IV fluids
-
Patients with burns larger than 20% of TBSA require IV fluid resuscitation because of GI ileus
-
For larger burns, the Parkland formula and its variations have become standard
-
Moderate burn victims should have at least 1 large-bore IV line placed through unburned skin
-
Severe burn victims should have at least 2 lines in place; if necessary, venous catheters may be placed through burned skin or via venous cutdown using the saphenous vein at the groin or ankle
-
When a burn patient requires considerable fluid resuscitation or has evidence of cardiopulmonary disease, a central venous line is indicated
-
In patients with massive burns or respiratory injury and elderly patients with severe burns or cardiac disease, fluid volume should be monitored with a pulmonary artery (Swan-Ganz) catheter
-
Administration of 5% albumin at 0.5 mL/kg/% TBSA, when endothelial integrity is restored 24 hours after the injury, replaces lost intravascular protein
-
A low-dose dopamine infusion (3-5 µg/kg/min) helps restore renal and splanchnic blood flow
-
Place a Foley catheter into the bladder to monitor the effectiveness of IV fluid replacement
-
In patients with major burn injuries who require IV fluid resuscitation, insert a nasogastric tube for initial evacuation of fluid and air from the stomach and feeding access
Calculation of fluid needs
All patients with a major burn injury must receive fluid resuscitation that is influenced by the percentage of the TBSA covered by the burn, [1] as well as by the presence of inhalation injury. Adequate resuscitation is evidenced by a normal sensorium, stable vital signs, and a normal urinary output, as follows:
-
Children younger than 2 years: 1 mL/lb/h
-
Older children: 0.5 mL/lb/h
-
Adults: ≥ 30-40 mL/h
The Parkland formula for calculating fluid needs for burn victims in the first 24 hours is as follows:
Fluid requirement (mL) = (4 mL of crystalloid) × (% TBSA burned) × body weight (kg)
An alternative formula for calculating fluid needs in children is the Galveston formula, by which the amount of lactated Ringer solution administered over the first 24 hours is determined as follows:
Fluid requirement = 5000 mL/m2 × % TBSA burned + 2000 mL/m2
Criteria for transfer to a burn center
The American Burn Association has established the following criteria for referring patients to a burn center [2] :
-
Any partial-thickness burn larger than 20% of total body surface area (TBSA) in a patient of any age or larger than 10% of TBSA in children younger than 10 years or adults older than 50 years
-
Third-degree burns covering more than 5% of TBSA
-
Second-degree or third-degree burns involving critical areas (eg, hands, feet, face, perineum, genitalia, or major joints)
-
Burns with associated inhalation injury
-
Electrical or lightning burns
-
Severe burns complicated by coexisting trauma - If traumatic injuries pose a higher risk to the patient than the burn injuries, the patient may have to be sent first to a trauma center
-
Preexisting disease that could complicate management of the burn injury
-
Chemical burns with threat of cosmetic or functional compromise
-
Circumferential burns on the extremities or the chest
Children with severe burns should be sent to a facility that has personnel and equipment to care for children with burns; children may be transferred between burn centers if the one they were originally brought to is not qualified or does not have the equipment required for the care of children. Patients with burns resulting from abuse may require long-term rehabilitative support.
Prehospital Treatment
Optimal management of burn victims is provided by an echelon system of burn care that is developed on a regional basis. Organization of burn care should begin at the site of injury and continue through prehospital care and transportation to the closest burn center, or to the closest emergency department (ED) with advanced life support capability, followed by transfer to a burn center when appropriate.
The immediate goal of prehospital treatment is to remove the person from the source of the burn. This must be accomplished without endangering rescue personnel. After extrication, initial care of the burn victim should follow the basic principles of trauma resuscitation (ie, airway, breathing, and circulation [ABCs]).
Burn victims rarely die immediately as a result of thermal injury; immediate death is typically the result of coexisting trauma or airway compromise. Accordingly, a rapid primary survey is performed to assess the ABCs. Any problems found should be corrected immediately. Any constricting clothing and jewelry should be removed to prevent these items from exerting a tourniquetlike effect after the development of burn edema.
When ventilatory and circulatory competence have been restored, a secondary survey is done. Concurrently with airway and circulatory management, emergency personnel must make an effort to stop the burning process.
Airway and breathing support
Fires usually emit smoke, which victims may inhale, especially in closed spaces. Smoke inhalation can cause both pulmonary parenchymal damage and carbon monoxide and other toxic poisonings, which may be life-threatening. [3, 4, 5]
Accordingly, during airway assessment, the prehospital care provider should look for signs of inhalation injury (eg, carbonaceous sputum, singed facial or nasal hairs, facial burns, oropharyngeal edema, vocal changes, or altered mental status). Inhalation injury should be assumed in anyone whose history suggests being confined in a fire environment.
If 1 or more of the signs of inhalation injury are present, humidified oxygen should be administered via a nonrebreathing reservoir mask or endotracheal tube at a rate of 10-12 L/min (see Smoke Inhalation; Carbon Monoxide Toxicity; and Prehospital Recognition and Management of Cyanide Poisoning in Smoke Inhalation Victims (Slides With Transcript)). A patient who is not breathing should be intubated and ventilated with 100% oxygen.
Treatment of burn shock
Treatment of burn shock in the prehospital setting should consist of elevating the patient’s legs 12 in. off the ground and administering humidified oxygen. If rescue personnel have advanced life support capability and transport time may be prolonged, these treatments are complemented by intravenous (IV) fluid administration.
Fluid resuscitation need not be initiated if patient will be transported to the hospital in less than 30 minutes. When the transport time will be longer than 30 minutes, the indications for fluid resuscitation include thermal injuries involving greater than 20% of total body surface area (TBSA) and evidence of burn shock.
Fluid resuscitation
Fluid administration should begin immediately with warmed fluid if possible. Catheters may be placed through burned skin if unburned skin is unavailable. If IV access is not possible, interosseous access methods may be considered. This is important because any burn extending over more than 15% of TBSA may produce shock as a result of hypovolemia. [6]
Fluid resuscitation is not recommended for children at the scene of the accident, because of the difficulties encountered in cannulating small veins. When fluid resuscitation is indicated in an adult, lactated Ringer solution or normal saline without glucose is administered through a large-bore percutaneous catheter, preferably inserted through unburned skin. The arm is the preferred site for cannulation. IV flow rates are determined according to the patient’s clinical status.
Cooling of burned tissue
Remove charred clothing. Immerse the burn wound in cold (1-5°C) water for about 30 minutes if transport cannot be undertaken immediately. This must be initiated as soon as possible: cooling has no therapeutic benefit if delayed more than 30 minutes after the burn injury. Do not use ice water, which may worsen the damage to the skin as well as promote hypothermia. [7] Do not apply ice directly to the burn wound: this may result in increased tissue injury through frostbite.
The beneficial effects of immediate cold water treatment of burned skin appear to be related to the following factors:
-
Cold inhibits lactate production and acidosis, thereby promoting catecholamine function and cardiovascular homeostasis
-
Cold also inhibits burn wound histamine release, which in turn blocks local and remote histamine-mediated increases in vascular permeability; this minimizes edema formation and intravascular volume losses
-
Finally, cold suppresses the production of thromboxane, implicated as the mediator of vascular occlusion and progressive dermal ischemia after burn injury
Local cooling of burns involving less than 9% of TBSA can be continued longer than 30 minutes to relieve pain; however, prolonged cooling of a larger burn can cause severe hypothermia, which may result in cardiac arrest. Prolonged irrigation with cool fluids or leaving the victim in wet sheets will not improve the burn and greatly increases the risk of hypothermia, as well as macerating the healthy tissues surrounding the burn.
Burn victims often complain of feeling chilled as a result of the loss of water and heat through the burned skin. Heat loss can be minimized by first placing a clean sheet under the patient and then covering the patient with another clean sheet, followed by clean blankets. The inside of the transport vehicle should be heated enough to make the patient comfortable. The goal is to “cool the burn wound but warm the patient.” [6]
Minor burns can be cooled with running tap water and dressed after more life-threatening issues have been addressed. It is important not to forget to provide the patient with adequate analgesia.
Transfer to burn center
If the vehicle with advanced life support capability can transport the burn patient to a specialized burn treatment facility within 30 minutes, the patient should be transferred directly to this facility, bypassing other hospitals. If the transport time to the specialized burn treatment facility is longer than 30 minutes, the patient should be transported instead to the nearest ED with advanced life support capability.
Initial Emergency Department Treatment
When the patient arrives in the emergency department (ED), perform a rapid initial assessment of respiratory and cardiovascular status, establish the extent and depth of burn injury (see the images below), and determine the need for special procedures. ED treatment focuses on airway and respiratory care and fluid resuscitation. [6, 8, 9, 10]
 Second-degree burns are often red, wet, and very painful. An enormous variability exists in their depth, their ability to heal, and their tendency to result in hypertrophic scar formation.
Second-degree burns are often red, wet, and very painful. An enormous variability exists in their depth, their ability to heal, and their tendency to result in hypertrophic scar formation.
 Third-degree burns are usually leathery, dry, insensate, and waxy. These wounds do not heal.
Third-degree burns are usually leathery, dry, insensate, and waxy. These wounds do not heal.
Most burns seen in the ED are minor. The key point in managing these wounds is to be sure that the patient receives adequate follow-up care. Cool the burn area with towels moistened with cool sterile saline. Avoid immersion in ice baths.
Burns of areas such as the face are best treated by means of an open technique. Wash the burn area, debride any open blisters, and cover the wounds with topical antibiotics. Fingers and toes should be wrapped individually, with fluffed gauze separating the digits in order to prevent maceration and adherence.
Cover all partial-thickness wounds with antibiotic ointment. Silver sulfadiazine is commonly used but may not be available to the emergency physician. Steroids have no role in treating burn wounds. Cleanse other areas with minor burns with the use of a mild soap and gentle scrubbing.
A debate exists as to whether intact blisters should be debrided (see the image below); the intact skin serves as a hermetic barrier, although the blister fluid can serve as an excellent medium for bacterial growth. Another argument for debridement is that removal of the blister roof allows topical agents to reach burn tissue. Blisters that are intact but are located in areas that have a high likelihood of rupture may be sharply debrided. The World Health Organization (WHO) recommends debridement of all bullae and excision of all adherent necrotic tissue. [11]
 Management of burn blisters is controversial. Many can be left intact to facilitate comfort while underlying wound heals. Sometimes, blisters obscure full-thickness wounds, as shown here, but, usually, wounds underlying blisters are partial-thickness wounds.
Management of burn blisters is controversial. Many can be left intact to facilitate comfort while underlying wound heals. Sometimes, blisters obscure full-thickness wounds, as shown here, but, usually, wounds underlying blisters are partial-thickness wounds.
Needle aspiration of the blisters should not be performed, because of the high risk of inoculating the blister with bacteria and thereby inciting infection. Open blisters should be debrided.
Wounds should then be treated with a topical antibiotic and dressed. Discharge the patient with explicit instructions on how to clean and dress the wound, and arrange follow-up care for evaluation of the wound.
Remember to check tetanus status of all patients and to administer tetanus immunization (Td) as appropriate. In addition, remember to place a nasogastric (NG) or orogastric (OG) tube in comatose patients, who tend to have gastric dilatation.
Intravenous (IV) antibiotics are not recommended in the initial treatment of most burn patients, because they may increase the chance of colonization with more virulent and resistant organisms. [7] These agents should be reserved for patients with secondary infections (notable as those with fever, malaise, or lymphangitis). Patients with secondary infections (see the images below) should also be admitted to the hospital because they may develop sepsis.
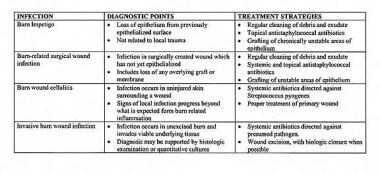
 Burn wound cellulitis presents with increasing erythema, swelling, and pain in uninjured skin around periphery of wound.
Burn wound cellulitis presents with increasing erythema, swelling, and pain in uninjured skin around periphery of wound.
 Invasive burn wound infection implies that bacteria or fungi proliferating in burn eschar are invading underlying viable tissues. These wounds display change in color, new drainage, and, commonly, foul odor. This infection can be life-threatening.
Invasive burn wound infection implies that bacteria or fungi proliferating in burn eschar are invading underlying viable tissues. These wounds display change in color, new drainage, and, commonly, foul odor. This infection can be life-threatening.
Airway and Respiratory Care
Inhalation injury has a significant impact on the survival of burn patients. It has 3 components: upper airway swelling, acute respiratory failure, and carbon monoxide intoxication. The natural history of upper airway burn injury is the development of edema that narrows the airway 12-24 hours after injury. Consequently, early intubation rather than observation is recommended in patients with signs of upper airway injury (eg, singed nasal hairs, facial burns, oral burns, sooty sputum, stridor, inspiratory grunting, wheezing, and tachypnea).
Fiberoptic bronchoscopy is a simple, safe, and accurate method of diagnosing acute inhalation injury; however, it often is not readily available to the emergency physician. Fiberoptic bronchoscopy reveals the anatomic level and severity of large airway injury; identification of supraglottic and infraglottic involvement is helpful in predicting ultimate pulmonary complications.
Fiberoptic bronchoscopy also may aid in intubating patients with inhalation injury. Because it has been associated with the development of severe hypoxemia, especially in elderly burn patients, supplementary oxygen should be administered through the bronchoscope. The ventilatory system for fiberoptic bronchoscopy can deliver a warmed, humidified, and measured fraction of inspired oxygen either for spontaneous or mechanically assisted ventilation (see below).
Once the airway is secured and the patient is oxygenated, further treatment includes maintenance of pulmonary toilet, relief of mechanical restriction of chest wall motion, and prevention of respiratory failure. When collagen is burned, it loses its elasticity, shortens its fibers, and becomes rigid. This can occur very quickly in fourth-degree and severe third-degree burns. When this process is combined with accumulation of burn edema in interstitial spaces, respiratory insufficiency or ischemia of an extremity may result.
The compressive effect of a full-thickness burn of the neck may contribute to airway compromise. Without tracheostomy, tight neck eschar accentuates pharyngeal edema and draws the neck into flexion, compressing the pharyngeal airway. A vertical incision through the eschar extending from the sternal notch to the chin helps maintain a patent airway.
If respiratory insufficiency is caused by a constricting eschar of the anterior thorax that limits respiratory excursion, escharotomy is imperative (see the images below). Lateral incisions are made in the anterior axillary lines that extend 2 cm below the clavicle to the ninth or 10th rib. The tops and bottoms of the incisions are then joined to form a square across the anterior chest.

Mechanical ventilation
If respiratory failure ensues, mechanical ventilation is necessary. Airway resistance is often increased after inhalation injury resulting from edema, debris within the airway, or bronchospasm. The goal of mechanical ventilation should be to accept a slightly acidic environment (pH > 7.32) so as to minimize the mean airway pressure required for ventilation. To keep airway pressures to a minimum, ventilator settings may have to be adjusted to slightly higher respiratory rates (16-20 breaths/min) and smaller tidal volumes (7-8 mL/kg).
Experimental studies of baboons with moderate smoke inhalation demonstrated that the barotrauma index (rate times pressure product) was significantly higher during regular ventilation than during high-frequency flow-interruption ventilation. Significantly greater histologic damage of pulmonary parenchyma also occurred in the group treated with conventional ventilation.
High-frequency flow-interruption ventilation appears useful with regard to its ability to recruit damaged, collapsed alveoli and keep them open in expiratory ventilation. Maintaining alveolar recruitment at low mean alveolar pressures helps minimize barotrauma and allows improved distribution of ventilation. Two retrospective studies demonstrated that the incidence of pneumonia and mortality in patients with inhalation injury was lower with high-frequency percussive ventilation than with conventional volume-limited ventilation.
Oscillating ventilator, which superimposes high-frequency ventilation on conventional tidal volume breaths, may be an even better method of ventilation after smoke injury. This method reduces barotrauma and aids in the removal of airway casts by causing vibratory air movement. Airway cast and plug formation can be decreased by nebulized heparin treatments (5000 U in 10 mL of normal saline every 4 hours), which inhibit fibrin clot formation in the airway.
Management of elevated carboxyhemoglobin
Carbon monoxide (CO) is present in smoke and has a 280 times greater affinity for hemoglobin than oxygen does. Obtain a CO level in all patients with suspected inhalation injury. Because the elimination half-life of carboxyhemoglobin (COHb) depends on oxygen tension, patients should receive 100% oxygen until their COHb level is lower than 10%.
In room air, the half-life of CO-bound hemoglobin is 4 hours. Under 100% oxygen, the half-life of CO-bound hemoglobin decreases to 45 minutes. Administration of 100% oxygen increases the gradient for oxygen binding to hemoglobin, and unbound CO is exhaled through the lungs.
Patients who have elevated COHb levels associated with a pH of less than 7.4 should be treated with hyperbaric oxygenation. Because serum COHb levels do not reflect tissue levels, evaluate relevant clinical symptoms when considering hyperbaric oxygen therapy. [12, 13] These symptoms include a history of unconsciousness, the presence of neuropsychiatric abnormalities, and the presence of cardiac instability or cardiac ischemia.
Management of cyanide poisoning
Specific therapy for cyanide poisoning in patients with inhalation injury is another consideration. Cyanide causes tissue hypoxia by uncoupling oxidative phosphorylation by binding to mitochondrial cytochrome a-a3. Consider empiric treatment for cyanide toxicity for patients with unexplained severe metabolic acidosis associated with elevated central venous oxygen content, normal arterial oxygen content, and a low COHb level.
Fluid Resuscitation
Establish intravenous (IV) access, and begin fluid resuscitation. Place 1 or 2 large-bore peripheral lines, and administer crystalloids. With the loss of the vapor barrier provided by intact skin, burn victims have large insensible fluid losses. Burn victims will need copious amounts of fluid because only 20-30% of it will remain in the intravascular space.
Patients with burn wounds smaller than 20% of total body surface area (TBSA) can be treated with a combination of oral and IV fluids. For larger burns, the Parkland formula (see below) and its variations have become the standard method for resuscitating the burned patient.
Moderate burn victims should have at least 1 large-bore IV line placed through unburned skin, and severe burn victims should have at least 2 lines in place. If necessary, venous catheters may be placed through burned skin or via venous cutdown using the saphenous vein at the groin or ankle.
When a burn patient requires considerable fluid resuscitation or has evidence of cardiopulmonary disease, a central venous line is indicated. Patients with massive burns or respiratory injury and elderly patients with severe burns or cardiac disease should be monitored with a pulmonary artery (Swan-Ganz) catheter to avoid fluid overload or inadequate replacement of volume.
Microvascular injury caused by a burn leads to increased vascular permeability with edema formation that results in ongoing plasma volume loss. Maximal edema formation occurs at 8-12 hours after burn injury for small burns and at 24-48 hours for large burns. The purpose of fluid resuscitation is to restore effective plasma volume, avoid microvascular ischemia, and maintain vital organ function. The amount of fluid required varies with the patient’s age, body weight, and percentage of TBSA burned.
Ideally, weigh the patient on a scale. In the absence of this measurement, obtain an estimate of the patient’s weight from the patient, a relative, or the patient’s driver’s license. Carefully map the burned areas over the entire body, including the back, to estimate fluid requirements during the first 48 hours after injury. Typically, burns larger than 20% of TBSA require IV fluid resuscitation because the accompanying gastrointestinal (GI) ileus precludes sufficient oral intake.
Calculation of fluid needs
All patients with a major burn injury must receive fluid resuscitation that is influenced by the percentage of the total body surface area (TBSA) covered by the burn (see the images below), [1] as well as by the presence of inhalation injury.
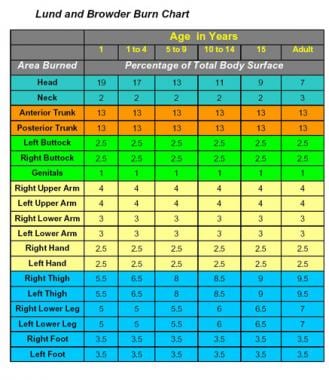 Lund and Browder chart illustrating method for calculating percentage of body surface area affected by burns in children.
Lund and Browder chart illustrating method for calculating percentage of body surface area affected by burns in children.
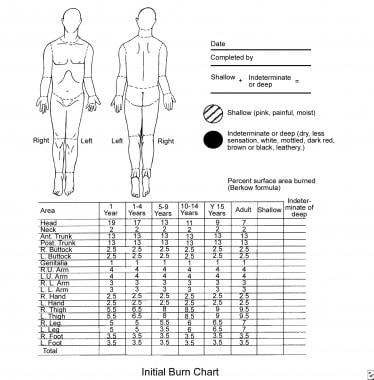 Size of burn is best estimated by using chart that corrects for changes in body proportions with aging.
Size of burn is best estimated by using chart that corrects for changes in body proportions with aging.
Several different formulas for fluid resuscitation have been recommended, although all emphasize that adequate resuscitation is evidenced by a normal urinary output (1 mL/lb/h in children younger than 2 years, 0.5 mL/lb/h in older children, and at least 30-40 mL/h in adults), a normal sensorium, and stable vital signs.
A survey of burn units in the United States and Canada found that 78% of the centers used the Parkland formula to estimate resuscitation volume and that lactated Ringer solution was the most popular type of fluid. [14] In marked contrast, a United Kingdom survey revealed that most burn units used human albumin solution and the Muir and Barclay formula to estimate resuscitation volumes. [2]
Since the publication of the findings of the Cochrane Injuries Group Albumin Reviewers, much discussion has ensued regarding the use of human albumin solution in patients who are critically ill. [15] In 2007, Baker et al reported that resuscitation of patients with thermal injuries in burn units in the United Kingdom and Ireland is fairly consistent with a shift toward crystalloid resuscitation and away from the use of human albumin solution. [16]
The Parkland formula for calculating fluid needs for burn victims in the first 24 hours is as follows:
-
Fluid requirement (mL) = (4 mL of crystalloid) × (% TBSA burned) × body weight (kg)
Thus, a man who weighs 70 kg and has a 30% TBSA burn would require 4 × 30 × 70 = 8400 mL in the first 24 hours.
One half of the calculated fluid requirement is administered in the first 8 hours, and the balance is given over the remaining 16 hours. Thus, fluids would be given at 525 mL/h for the first 8 hours, then at 262.5 mL/h for the remaining 16 hours. It is important to calculate fluid loss from the time of injury, as well as to take into account the fluid administered by prehospital personnel for fluid replacement.
Monitor typical markers of fluid status (eg, urine output) and adjust fluids accordingly. Placement of a Foley catheter (see below) simplifies monitoring of hourly urine output. Urine output should be maintained at 0.5 mL/kg/h.
Strict adherence to a formula for fluid resuscitation does not guarantee successful fluid therapy. For example, the Parkland formula does not predict fluid resuscitation needs in electrical injuries accurately, and the presence of coexisting trauma may increase fluid volumes needed for resuscitation.
If the need is expected to exceed 6 mL/kg times the percentage of TBSA burned per 24 hours, if the patient appears unresponsive to resuscitation, or if signs of impending cardiac failure are present, insertion of a pulmonary artery (Swan-Ganz) catheter for measurement of pulmonary artery pressure and cardiac output is advisable. If the volume is found to be adequate but urine output remains diminished, then dopamine (5 µg/kg/min) may be used to increase renal perfusion.
During resuscitation, the most common error is overhydration, which increases the risk of acute respiratory distress syndrome (ARDS) developing 3-5 days after the burn. In patients with concomitant large TBSA burns and inhalation injury, the Parkland formula may result in unnecessarily large fluid loads. To avoid overhydration, resuscitate patients who have inhalation injuries with amounts substantially lower than specified by the formula, accepting a urinary output in the range of 0.3-0.5 mL/kg/h.
Replacement of lost protein
After a burn injury, a substantial amount of intravascular protein is lost through endothelial leaks in the burned vessels. When endothelial integrity is restored 24 hours after the injury, some clinicians favor the administration of 5% albumin at 0.5 mL/kg/% TBSA to maintain dynamic forces between the extracellular spaces and the intravascular system. In addition, a low-dose dopamine infusion (3-5 µg/kg/min) is beneficial in restoring renal and splanchnic blood flow in patients with major burn injury.
Catheterization and intubation
Place a Foley catheter into the bladder to monitor the effectiveness of IV fluid replacement. Burns of the perineum also are best cared for with an indwelling Foley catheter to decrease urinary soiling of the wound.
In patients with major burn injuries who require IV fluid resuscitation, pass a nasogastric (NG) tube for initial evacuation of fluid and air from the stomach and feeding access. Removal of the gastric contents prevents vomiting and aspiration, sequelae of the ileus that commonly occur soon after burn injuries involving more than 20% of TBSA. Early feeding through the NG tube within 6-8 hours of the burn injury diminishes the hypermetabolic response and maintains intestinal integrity.
Hypertonic saline solutions
Resuscitation with hypertonic saline solutions reduces the fluid volume required. The volume of fluid administered using hypertonic fluid solutions is notably less, yet fluid requirements and percent weight gain have not been shown to be lower with hypertonic saline than with Ringer solution. The anticipated benefits of fewer escharotomies and limited ileus have not been uniformly encountered either.
On the contrary, hypertonic saline resuscitation has been associated with an increased incidence of acute tubular necrosis and hyperchloremic metabolic acidosis, which can exacerbate the metabolic acidosis of hypovolemic shock. Therefore, hypertonic saline is not currently recommended for resuscitation of burn patients.
Decision not to resuscitate
When a patient with a major burn injury is extremely unlikely to survive (eg, an elderly patient in whom more than 80% of the TBSA is burned), the clinician must be encouraged not to begin fluid resuscitation. This decision must be made only after thoughtful discussion with family members. When resuscitation is not undertaken, the clinician must ensure that patients are not in pain, keep them warm, and allow them to remain in a room with family members.
Special considerations in children
In most respects, burn care in children is similar to that in adults; however, there are some relevant physiologic differences that must be considered in the care of burned children.
Differences in TBSA-weight ratio
The Parkland formula is effective in estimating fluid loss in adults, but it underestimates the evaporative fluid loss and maintenance needs in children. Compared with adults, children have a larger TBSA relative to weight and generally have somewhat greater fluid needs during resuscitation.
An alternative formula that is preferred by many for calculating fluid needs in children is the Galveston formula, which is based on TBSA rather than body weight. Although many pediatric burn centers believe that this formula is more accurate than the Parkland formula, it is more time-consuming to calculate.
By the Galveston formula, the amount of lactated Ringer solution administered over the first 24 hours is determined as follows:
Fluid requirement = 5000 mL/m2 × % TBSA burned + 2000 mL/m2
One half of the total fluid is given in the first 8 hours, with the balance given over the next 16 hours. The maintenance fluid should then be lactated Ringer solution with 5% dextrose; the dextrose is added to the resuscitation fluid to prevent hypoglycemia because children have smaller glycogen stores than adults do.
In children, keep the urine output at 1 mL/kg/h, the pulse in the range of 80-180 beats/min (depending on age), and the base deficit lower than 2.
Differences in thermoregulation
In infants younger than 6 months, temperature is regulated by nonshivering thermogenesis, a metabolic process by which stores of brown fat are catabolized under the influence of norepinephrine, which requires large amounts of oxygen. Consequently, prolonged hypothermia in burned infants may result in excessive lactate production and acidosis.
After 6 months, infants and children are able to shiver. Because they have greater evaporative water loss relative to weight than adults do, infants and children are especially prone to hypothermia; therefore, keep the ambient temperature high to decrease radiant and evaporative heat loss from burned infants and children to the environment.
Differences in renal function
Differences in renal function between infants and adults may have important therapeutic implications for the treatment of burned children. The glomerular filtration rate in infants does not reach adult levels until the age of 9-12 months, because of an imbalance in maturation of tubular and glomerular functions. During this early period, infants have approximately half the osmolar concentrating capacity of adults, and a water load is handled inefficiently.
The rate of water excretion is time dependent and decreases as water loading continues. During the first several weeks of life, infants are likely to retain a larger portion of a water load administered as part of burn resuscitation. The hyposmolarity of lactated Ringer solution, when used in accordance with the Parkland formula, already accounts for the free water needs of infants during the first 24 hours after the burn. Additional water often results in fluid overloading.
Treatment of Special Burn Types
Tar burns
The boiling points of asphalt and roofing tar are 140° C and 232° C, respectively. Tar cools rapidly to between 93°-104° C as soon as it leaves the heat source. In most cases, the tar is cool by the time the patient arrives in the emergency department (ED). If it is not, it should be actively cooled to terminate thermal damage with room temperature saline or water.
Once the tar is firm, it should be picked, peeled, and debrided from the underlying tissue. Some degree of autodebridement will occur. Debridement involves a balance between removing the foreign body (tar) and exposing the injured skin for evaluation and treatment. Judgment should be exercised as to how much debridement is appropriate in the emergency setting. Extensive debridement may necessitate moderate-to-deep sedation.
If the skin has only a light coating of tar and the patient does not complain about the underlying skin or surrounding tissue, leaving the tar in place may be acceptable. Tar that is part of an obvious burn, blister, or tissue loss should be removed. Tar on the conjunctiva should be removed by an ophthalmologist.
Applying ointments, such as polymicrobial antibiotic ointment, petroleum jelly, or mineral oil, can facilitate tar removal. Organic solvents, such as acetone or gasoline, must be not be used to remove the tar. If an ointment is used, it should be left on for 2-4 hours at a time until the tar has dissolved.
Common household agents, such as mayonnaise, butter, sunflower seed oil, and baby oil, have been promoted for removal of tar. Organic, nonsterile agents are easy to acquire and are available in large quantities, but they carry the risk of promoting wound infection or allergic reaction. Bacterial or fungal growth can occur if the tar is not completely removed and the organic agent is not completely rinsed off.
Recently published guidelines for the treatment of asphalt burns recommend immediate cooling, gradual removal of adherent asphalt with topical antibiotics, and avoiding use of topical agents that may cause tissue toxicity. Standard burn management should be performed once the asphalt is removed. In addition to topical antibiotics, other solvents used to remove asphalt include petroleum jelly, sunflower oil, baby oil, liquid paraffin, butter, mayonnaise, and Moist Exposed Burn Ointment. Use of kerosene, gasoline, or ethanol can damage tissue. [17, 18]
Circumferential full-thickness burns involving extremities
Circumferential full-thickness burns involving the extremities or the chest may warrant escharotomy. As edema forms in the injured extremity after the burn, the tough, rigid eschar restricts outward expansion of the tissue, and the interstitial pressure rises to the point where vascular flow is compromised. In short, the eschar behaves like a tourniquet. This typically occurs 12-24 hours after an injury. Incising the eschar allows return of flow and prevents further ischemic injury. Because full-thickness burns are insensate, topical anesthetics are not needed.
Perform escharotomy along the lateral aspect of the extremity with a linear and lengthwise incision. Use of an electrocautery simplifies the procedure and can reduce the amount of bleeding. The incision should go completely through the eschar. The subcutaneous fat will appear to bubble up into the escharotomy wound. Bleeding is minimal and is easily controlled by pressure. Upon completion of the escharotomy, a dressing with antibiotics is placed on the wound, and the extremity is elevated to help maintain homeostasis.
If the chest is involved and the eschar compromises ventilatory motion, perform an escharotomy involving the anterior chest. Incisions are made along the costal margin, along the anterior axillary lines, and across the top of the chest, freeing up the anterior chest wall.
Criteria for Transfer to Burn Center
The American Burn Association has established the following criteria for referring patients to a burn center [2] :
-
Any partial-thickness burn larger than 20% of total body surface area (TBSA) in a patient of any age or larger than 10% of TBSA in children younger than 10 years or adults older than 50 years
-
Third-degree burns covering more than 5% of TBSA
-
Second-degree or third-degree burns involving critical areas (eg, hands, feet, face, perineum, genitalia, or major joints)
-
Burns with associated inhalation injury
-
Electrical or lightning burns
-
Severe burns complicated by coexisting trauma - If traumatic injuries pose a higher risk to the patient than the burn injuries, the patient may have to be sent first to a trauma center
-
Preexisting disease that could complicate management of the burn injury
-
Chemical burns with threat of cosmetic or functional compromise
-
Circumferential burns on the extremities or the chest
Children with severe burns should be sent to a facility that has personnel and equipment to care for pediatric burn cases. Children may be transferred between burn centers if the one they were originally brought to is not qualified or does not have the equipment required for the care of children. With burns that result from abuse, the patient may require long-term rehabilitative support
Before transfer, the referring physician must ensure adequate respiratory support, as follows:
-
If the patient is at risk for airway compromise or deterioration, perform intubation prior to transfer [19]
-
Support with 100% oxygen
-
Stabilize circulatory status by means of fluid resuscitation
-
Administer Ringer solution at the rate indicated by the Parkland formula or at that rate adjusted for clinical status (eg, urine output)
-
Ensure adequate vascular access for fluid resuscitation and administration of analgesics, if necessary
-
Give transporting personnel orders defining the rate and amount of analgesics that can be administered during transport
The referring physician must also ensure appropriate care of the burn wound, as follows:
-
Cover patients being transferred with a dry sheet
-
Transport crews should exercise care to prevent the patient from becoming hypothermic
-
Use of saline-soaked dressings increases risk of hypothermia
-
Application of antimicrobial creams may delay transfer, and these agents must be removed once the patient arrives at the burn center
Physician-to-physician contact before transfer is essential. The accepting physician at the burn center can provide advice on caring for the burn patient and often can assist in arranging transfer. Documentation of the care already provided for the patient and of any relevant findings should accompany the patient to the burn center.
Guidelines
Clinical practice guidelines on the management of acute pain in the adult burn patient were released in September 2020 by the American Burn Association. [20]
Elements of the pain assessment are as follows:
-
Perform several times daily.
-
Follow a protocol to ensure consistency in language.
-
If able, use pain assessment tools: patient-reported scales, Burn Specific Pain Anxiety Scale (BSPAS), Critical Care Pain Observation Tool (CPOT).
For opioid pain medications, the choice should be based on physiology, pharmacology, and physician experience. It should be individualized to the patient, with frequent adjustments to account for individual patient responses, the narrow therapeutic effects, and adverse effects. Use as few opiate equivalents as necessary for successful pain control. They should be used together with nonopioid and nonpharmacological measures. Educate patients about opioids and other pain medications and their roles in recovery.
The roles of nonopioid pain medications are as follows:
-
Acetaminophen: Use on all burn patients; monitor maximum daily dose.
-
NSAIDs: Consider use, owing to safety profile and efficacy; factors to consider include patient clinical picture (comorbidities) and surgeon preference.
-
Neuropathic pain agents (eg, gabapentin, pregabalin): Consider as adjuncts to opioids in those with neuropathic pain or whose pain is refractory to standard therapy.
-
Ketamine: Consider use for procedural sedation or in low doses as an adjunct to opioids in those who in whom reduced opioid consumption would be beneficial, in particular postoperatively.
-
Dexmedetomidine and clonidine: Recommended as pain management adjuncts; particular scenarios include patient signs of withdrawal and/or prominent anxiety; dexmedetomidine is a first-line choice for intubated burn patients.
-
Intravenous lidocaine: Not recommended as a first-line agent; however, it can be considered as a second- or third-line adjuvant.
-
Cannabinoids: Not recommended, owing to lack of evidence along with potential legal and political obstacles.
The use of regional anesthesia for burn pain management can potentially achieve improved pain relief, improved patient satisfaction, and a reduction in opioid use, without serious risks or complications.
Nonpharmacologic pain control techniques should be offered to every patient. The modalities for which the strongest evidence exists are hypnosis, cognitive-behavioral therapy, and virtual reality.
-
Partial- and full-thickness burns from a structure fire. Note facial involvement.
-
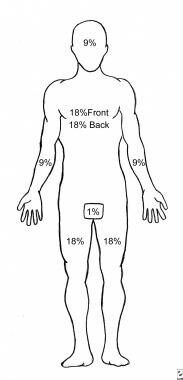
Rule of nines for calculating burn area.
-
Lund and Browder chart illustrating method for calculating percentage of body surface area affected by burns in children.
-
Child with burns from scalding. Hot soup was spilled when child grabbed handle of pot. Note full-thickness burn to left upper part of chest. Edema of lips and blisters on face and nose indicate second-degree burns of face.
-
Escharotomy to release chest wall and allow ventilation of patient.
-
59-year-old physician with deep-seated bulla on middle finger after burning himself taking a hot bun out of the oven.
-
The American Burn Association has developed criteria for burn center transfer. These criteria have been adopted by most emergency medical services.
-
Size of burn is best estimated by using chart that corrects for changes in body proportions with aging.
-
Second-degree burns are often red, wet, and very painful. An enormous variability exists in their depth, their ability to heal, and their tendency to result in hypertrophic scar formation.
-
Third-degree burns are usually leathery, dry, insensate, and waxy. These wounds do not heal.
-
Management of burn blisters is controversial. Many can be left intact to facilitate comfort while underlying wound heals. Sometimes, blisters obscure full-thickness wounds, as shown here, but, usually, wounds underlying blisters are partial-thickness wounds.
-
Clinically focused definition set describing burn wound infections.
-
Burn wound cellulitis presents with increasing erythema, swelling, and pain in uninjured skin around periphery of wound.
-
Invasive burn wound infection implies that bacteria or fungi proliferating in burn eschar are invading underlying viable tissues. These wounds display change in color, new drainage, and, commonly, foul odor. This infection can be life-threatening.
-
Large (and increasing) numbers of medications and membranes have been selected for use in burn wound management.
-
If hand positioning and therapy are ignored while overlying burns heal, long-term suboptimal function may result.
-
Depth of partial-thickness burns is routinely underestimated in outpatient setting.
-
Two-year-old child is brought to office for evaluation of scald burn to hand.
-
Splinting of serious hand burn.








