Practice Essentials
Imperforate hymen is a congenital anomaly of the female genital tract in which the hymen completely obstructs the vaginal opening. [1] It is the most common and most distal form of vaginal outflow obstruction. As a consequence of normal development, the central portion of the hymenal membrane is usually absent. This absence creates the typical configuration of a ringlike structure at the level of the vaginal vestibule. Persistence of the intact hymenal membrane results in the condition of imperforate hymen.
Thorough genitourinary examination is essential in girls of all ages from birth through the onset of menarche. If primary amenorrhea is identified or if other structural abnormalities are noted, proper management is essential. By performing these examinations and by promptly diagnosing and treating imperforate hymen, primary care practitioners can help prevent the obstructive symptoms of imperforate hymen and its potential high-risk complications due to delayed care. [2, 3, 4, 5]
After appropriate evaluation is completed to exclude complicated obstruction of the vaginal tract outflow, management of imperforate hymen is straightforward. Medical therapy has no role in the management of imperforate hymen, because the retained secretions are typically sterile. In addition, the hymen must be surgically resected to relieve the obstruction. Long-term complications are minimal.
For patient education resources, see the Women's Health Center, as well as Amenorrhea and Female Sexual Problems.
Anatomy
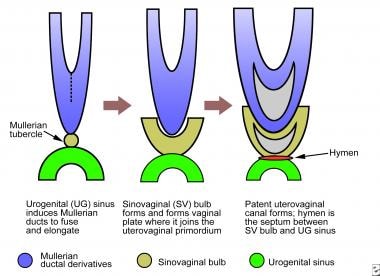
The hymen originates from the embryonic vagina buds from the urogenital sinus. As a consequence, the hymen is a composite of vaginal epithelium and epithelium of the urogenital sinus interposed by mesoderm. Once the hymen becomes perforated or forms a central canal, it establishes a communication between the upper vaginal tract and the vestibule of the vagina (see the image below). [6]
The imperforate hymen is a solid membrane interposed between the proximal uterovaginal tract and the introitus. Ambroise Paré first described this condition in 1633. [7] It is classified as a vertical fusion defect. However, it differs from other vertical fusion defects in that it is not derived from the müllerian system. The configuration and normal size of the hymenal orifice in prepubertal girls has received attention in the context of evaluating potential child abuse. [8]
Anatomic variations of the patent hymen exist, with the most common being an anular or circumferential hymen in which the hymen completely surrounds the vaginal orifice and has a central opening. Other appearances of the hymen include crescentic, fimbriated, septate, cribriform, and microperforate forms. In some patients, perforations do not become confluent, and a cribriform pattern with multiple small perforations may be observed. [9]
Vaginal abnormalities in the premenarchal patient include hymenal and vaginal cysts, urethral prolapse, labial agglutination, vaginitis, foreign bodies, and lichen sclerosis.
Pathophysiology
Any obstruction of the vaginal tract during the antenatal, perinatal, or adolescent period results in the entrapment of vaginal and uterine secretions. In patients with imperforate hymen, this obstruction is at the level of the introitus and becomes evident when the distensible membrane bulges between the labia. Various terms, such as mucocolpos, hematocolpos, and pyocolpos, are used to describe this condition, depending on the nature of the retained contents.
In fetal development and in the immediate perinatal period, mucoid secretions from the uterovaginal tract result in mucocolpos under the influence of maternal estrogens. When the diagnosis is made in adolescence, the retained secretions consist of menstrual products, and the resulting mass effects in the vagina and uterus are referred to as hematocolpos and hematometrocolpos, respectively. Reflux of the endometrial tissue through the fallopian tubes (ie, hematosalpinx) may result in secondary endometriosis.
An accumulation of infected material within the vaginal cavity (ie, pyocolpos) may result from an infection that is ascending through microperforations in the membrane.
Etiology
Specific etiologies for the failure to establish patency are not evident. The cause may be related to failure of apoptosis due to a genetically transmitted signal, or it may be related to an inappropriate hormonal milieu. Familial inheritance in successive generations has been described. [10]
Epidemiology
Imperforate hymen is the most frequent cause of vaginal outflow obstruction, occurring in 0.05-0.1% of infant girls. [1]
Prognosis
Outcome after repair of imperforate hymen is excellent. If findings on an appropriate preoperative evaluation are normal, a patient can be reassured that her genital tract is otherwise normal. The incidence of dyspareunia is also low.
-
Embryologic origin of the hymenal membrane.
-
Neonate with a bulging perineum due to mucocolpos.
-
Sagittal sonogram in an adolescent with imperforate hymen shows a distended vagina and uterus.
-
Transverse sonogram in an adolescent with imperforate hymen shows a distended vagina immediately posterior to the bladder.




