Background
Conjoined twinning is one of the most fascinating human malformations and has also been reported in other animals—mammals, fishes, birds, reptiles, and amphibians. [1, 2, 3, 4] The term Siamese twins, once commonly used for conjoined twins, has fallen out of favor because it seems to convey that these individuals are circus freaks or monsters. Conjoined triplets have been described but are quite rare. [5]
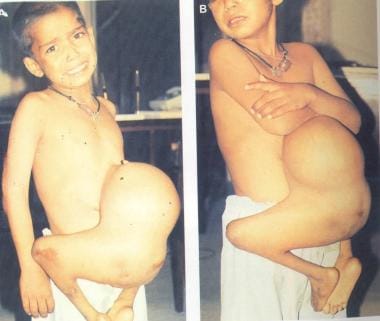
The major types of conjoined twins were described in 1573 by the French renaissance surgeon Ambroise Pare. Approximately 75% of conjoined twins are female, and 70% are fused at the thorax (thoracopagus) or abdomen (omphalopagus). The union can be in the frontal, transverse, or sagittal plane. The following two photographs show union in a transverse plane in the lower body area, so that the twins face each other.
 Union in a transverse plane in the lower body area, so that the twins face each other.
Union in a transverse plane in the lower body area, so that the twins face each other.
 Union in a transverse plane in the lower body area, so that the twins face each other.
Union in a transverse plane in the lower body area, so that the twins face each other.
The two main categories of conjoined twinning are as follows:
-
Symmetrical or equal conjoined twins (ie, two well-developed babies)
-
Asymmetrical or unequal conjoined twins (ie, a small part of the body is duplicated, or an incomplete twin is attached to a fully developed twin)
In broad terms, conjoined twins may be regarded as a doubling anomaly. The later the incomplete embryologic separation occurs, the higher the likelihood of a complicated fusion.
Treating conjoined twins can be a daunting challenge for the surgeon.
Successful separation of a set of omphalopagus twins was first reported in 1689 in Basel, Switzerland. [6] Whereas series of experience with conjoined twins have been reported in the literature, [7, 8, 9] successful separation of large numbers of conjoined twins has been limited to a few centers in the world, including the following:
-
13 sets described by O'Neill et al from the Children's Hospital of Philadelphia in 1988 [10]
-
14 sets reported by Mackenzie et al from the same hospital in 2002 [11]
-
17 sets reported by Spitz and Kiely in the same year from the Great Ormond Street Hospital, London [12]
-
46 sets reported by Rode et al from Red Cross Children's Hospital, Cape Town, South Africa [13]
Surgical experience with conjoined twins has also been reported in other parts of the world, such as China, Saudi Arabia, and New Zealand. [14, 15, 16]
In Singapore in 2003, skull and brain separation of 29-year-old craniopagus Iranian twins, Ladan and Laleh Bijani, was unsuccessful, and the sisters died of exsanguination on the operating table.
Craniopagus conjoined twins Mohamed and Ahmed Ibrahim, born in Egypt on June 2, 2001, were separated at the Children's Medical Center in Dallas, TX, on October 12, 2003, during a 34-hour operation. The operation involved skin grafting and separation of the venous sinuses. Later, they underwent skull reconstructive surgery, received rehabilitation therapy, and, finally, left for Egypt on November 19, 2005. A successfully staged separation of craniopagus twins (Carl and Clarence Aguirre) took place from 2003 to 2004 at Montefiore Medical Center in New York.
Cases of conjoined twinning often give rise to religious, [17] moral, ethical, [18] and legal [19, 20, 21] concerns. For example, in England, the separation of a pair of conjoined twins from Malta, born August 8, 2000, raised considerable ethical and legal issues. [22] The parents refused to grant permission for surgery, and the matter was referred to court. The judges concluded that separation was in the best interests of both children, even though it meant the death of the weaker twin. In the United States, the decision of the parents might have been final.
A support group for conjoined twins, Conjoined Twins International, was founded in 1996 in Prescott, Arizona, by the grandparents of a set of conjoined twins. Facebook also has a support circle of friends of conjoined twins. In addition, blog sites have been set up for certain sets of twins.
Pathophysiology
The morula becomes a blastocyst on day 6 after the ovum is fertilized. An inner cell mass develops at one end within this vesicle. The inner cell mass can form a whole fetus. Conjoined twins are produced when this inner cell mass, derived from a single zygote, incompletely splits late, after the 12th day of gestational life (see the image below).
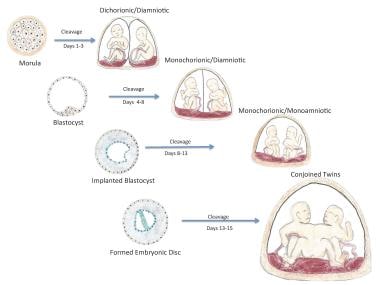 The term conjoined twinning refers to an incomplete splitting of monozygotic twins after 12 days of embryogenesis. Image created by Samantha Cloutier and Aaron Cloutier.
The term conjoined twinning refers to an incomplete splitting of monozygotic twins after 12 days of embryogenesis. Image created by Samantha Cloutier and Aaron Cloutier.
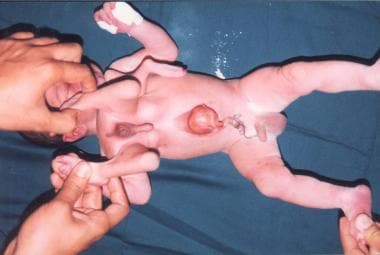
The delivered fetuses are physically joined at some point as a result. The larger the connecting bridge between the twins, the more complex its contents. Conjoined twins are classified according to their point of union is used to classify twins; the terms used include the Greek word pagos, which means "that which is fixed" (see Presentation). An especially rare condition occurs when one incompletely formed (ie, parasitic) twin is dependent on the well-formed one. This is known as heteropagus twinning. (See the images below.)
 This is a much more rare occurrence termed heteropagus twinning. One twin is not fully formed (parasitic twin) and is dependent on the well-formed one. A malformed head, upper limb, and large ears are present in the parasitic twin. Three legs (tripus) are present.
This is a much more rare occurrence termed heteropagus twinning. One twin is not fully formed (parasitic twin) and is dependent on the well-formed one. A malformed head, upper limb, and large ears are present in the parasitic twin. Three legs (tripus) are present.
 Ethical issues arose in this set. The parents refused separation on the basis that the nonviable twin was still breathing. The wishes of the parents were respected. This set of twins was lost to follow-up.
Ethical issues arose in this set. The parents refused separation on the basis that the nonviable twin was still breathing. The wishes of the parents were respected. This set of twins was lost to follow-up.
Another example of parasitic twin, in which the head is not visible, and the ethical decision is easier to make, is shown below.

A nonoperated case of parasitic twins, presenting late, is shown below.
The parasitic twin (sacrificed) after separation is shown below.

Multiple limbs attached to the thorax are shown below.
Etiology
The incomplete anatomic separation between monozygotic twins occurs sporadically, with no increased risk in future pregnancies.
Seven cases (two published) have been reported in which conjoined twinning occurred with the use of clomiphene for induction of ovulation. Two cases of thoracopagus have been reported in which conjoined twinning occurred with periconceptional maternal griseofulvin intake. Spina bifida is associated with conjoined twinning, and one case of conjoined twinning after maternal exposure to valproic acid has been reported.
No gene mapping or linkage analysis currently exists for the malformation. Some investigators implicate abnormal X inactivation. The latter may be related to the increased incidence in female twins. Other studies refute abnormal X-chromosome inactivation.
Epidemiology
Twinning occurs in approximately 1 of every 87 live births. Monozygotic twins account for one third of twin births. Conjoined twins account for 1% of monozygotic twins. In the United States, the incidence is 1 per 33,000-165,000 births and 1 per 200,000 live births. [23] The stillbirth rate is 40-60%. More cases are being reported now because of the routine use of fetal ultrasonography (US).
The condition is probably more common in Indian and African populations than in Whites. Exact epidemiology across different races and nations is not known because of underreporting and lack of facilities for antenatal diagnosis.
When born live, females are affected more often than males, with a female-to-male ratio of 3:1 or greater. Stillborn conjoined twins are predominantly male.
Conjoined twins show characteristic points of attachment. They are classified according to the site of union, with the following frequency:
-
Thoracoomphalopagus (ie, joined at the chest, abdomen, or both), 74% - Thoracopagus or xiphopagus (ie, joined at the chest), 40%; omphalopagus (ie, joined at the abdomen; see the first and second images below), 34%
-
Pygopagus (ie, joined at the buttocks), 18%
-
Ischiopagus (ie, joined at the ischium), 6%
-
Craniopagus (ie, joined at the head; see the third and fourth images below), 2%


 A radiograph of the skull, showing the conjoined heads in the case in previous two images.
A radiograph of the skull, showing the conjoined heads in the case in previous two images.
Magnetic resonance imaging (MRI) or computed tomography (CT) may show the brain structure, whereas magnetic resonance angiography (MRA) can show the extent of vascular connections (see the image below).
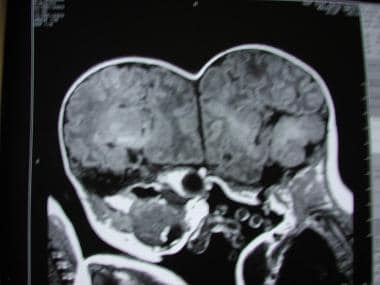 An MRI or CT may show the brain structure, while a magnetic resonance angiography can show the extent of vascular connections.
An MRI or CT may show the brain structure, while a magnetic resonance angiography can show the extent of vascular connections.
Prognosis
Several factors may predict or influence outcome, including the following:
-
Antenatal MRI and echocardiography - These techniques can be performed to accurately define the conjoined anatomy, and an outcome can be predicted, though the echocardiogram can underestimate the complexity of the cardiac anatomy; although 9 weeks is the earliest gestational age at which conjoined twins have been detected, false-positive cases are common before 10-11 weeks, as the fetal movements are limited; monoamniotic twins may appear conjoined
-
Postnatal surgery - Generally, the twins are separated at age 6-12 months, and the prognosis improves with elective surgery and meticulous preoperative planning; cardiac anatomy occasionally necessitates urgent separation at birth; however, urgent operations carry a high (40-80%) mortality
-
Skin closure material - Use of skin expanders and prosthetic mesh has improved outcome through providing better wound closure; however, use of prosthetic mesh for abdominal closure often results in fistula formation
-
Thoracopagus with cardiac conjunction - The prognosis for separating twins with conjoined ventricles remains poor, unless two cadaveric cardiac transplants were made available; only one case of successful separation of conjoined atria has been reported; factors associated with increased survival include elective separation, older age, and cardiac conjunction involving only shared pericardium [24]
-
Craniopagus - Usually, the twins have two largely separate brains; however, the venous sinus may be shared, and division of this sinus carries a high risk for life-threatening exsanguination
-
This set of conjoined twins was a stillbirth. Prenatal ultrasonography failed to reveal the second head. An emergent cesarean section was performed after failure to progress.
-
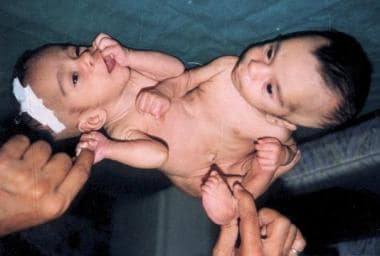
This is an example of double-headed (bicephalus) conjoined twins, a rare occurrence.
-
Even though conjoined twinning is more common in female fetuses (75% of cases), most stillborn conjoined twins are male. A single penis and 2 testes were present in this case.
-
This is a much more rare occurrence termed heteropagus twinning. One twin is not fully formed (parasitic twin) and is dependent on the well-formed one. A malformed head, upper limb, and large ears are present in the parasitic twin. Three legs (tripus) are present.
-
Ethical issues arose in this set. The parents refused separation on the basis that the nonviable twin was still breathing. The wishes of the parents were respected. This set of twins was lost to follow-up.
-
Conjoined twins unified at the thorax and abdomen.
-
Another view of the same set of twins as shown in the previous image.
-
A superior radiographic view of the same set of twins as shown in the previous 2 images. The twins have 2 hearts that are not conjoined, making this a possible operation.
-
Esophagram showing union at the level of stomach.
-
Ischiopagus tetrapus twins.
-
Ischiopagus tripus twins.
-
Thoracoomphalopagus twins.
-
Pygopagus twins.
-
Ischiopagus tetrapus twins.
-
Craniopagus twins.
-
Craniopagus twins.
-
Rachipagus twins.
-
Parapagus twins.
-
Pygopagus twins.
-
Cephalothoracopagus twins.
-
Ischiopagus tetrapus twins.
-
Omphalopagus twins.
-
Thoracopagus twins.
-
Parasitic twinning.
-
Union in a transverse plane in the lower body area, so that the twins face each other.
-
Union in a transverse plane in the lower body area, so that the twins face each other.
-
The term conjoined twinning refers to an incomplete splitting of monozygotic twins after 12 days of embryogenesis. Image created by Samantha Cloutier and Aaron Cloutier.
-
An example of parasitic twin, in which the head is not visible.
-
A nonoperated case of parasitic twins, presenting late.
-
The parasitic twin (sacrificed) after separation.
-
Multiple limbs attached to the thorax.
-
Omphalopagus twins.
-
Omphalopagus twins.
-
Craniopagus twins.
-
A radiograph of the skull, showing the conjoined heads in the case in previous two images.
-
An MRI or CT may show the brain structure, while a magnetic resonance angiography can show the extent of vascular connections.
-
A case of thoracoomphalopagus twins, after separation.
-
Thoracoomphalopagus twins.





