Practice Essentials
Cystic dilatation of the common bile duct (CBD), also known as choledochal cyst, is a fairly uncommon anomaly of the biliary tract. With the use of antenatal ultrasonography (US), an increasing number of choledochal cysts have been reported in the fetus. [1, 2, 3, 4, 5, 6, 7] Incomplete gastric obstruction by a large cyst is one of the typical clinical manifestations in newborns and young infants. [8] The earliest reported choledochal cyst was detected in a fetus at 15 weeks' gestation, which may correspond to the timing of the formation of pancreatic enzymes.
Antenatal demonstration of a cystic structure inferior to the liver strongly suggests the diagnosis. Fetal development should be carefully monitored with serial US after such a discovery. Most centers prefer to excise the cyst shortly after birth. A waiting period of a few weeks is necessary to stabilize the baby and allow for proper preoperative evaluation. [9] Surgical excision in the neonatal period has been shown to be technically feasible and well tolerated by the patient.
The management of choledochal cysts has evolved during the past several decades. [10] Complete excision of the cyst and biliary bypass have become the treatment of choice. Other procedures, such as cystoduodenostomy or cystojejunostomy, have been associated with high morbidity and the potential for malignant transformation in the residual cyst. Even after complete excision, sporadic cases of cancer in the remaining biliary tree have been reported.
Anatomy
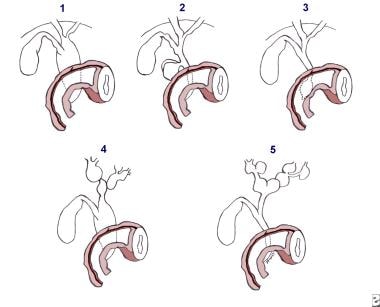
In 1959, Alonso-Lej et al defined three types of choledochal cyst, [11] and in 1977, Todani et al modified this classification by adding two new types (IV and V). [12] (See the image below.) Others have subsequently added further subtypes on the basis of cholangiographic findings. The five types described by Todani are as follows:
-
Type I - Cystic or fusiform dilatation of the common bile duct (CBD); most frequent type (90-95% of cases).
-
Type II - Diverticulum of the CBD, with normal-sized CBD
-
Type III - Choledochocele, a cystic dilatation of the distal intramural portion of the CBD, typically protruding into the second portion of the duodenum
-
Type IV - Cystic or fusiform dilatation of the CBD associated with cystic, fusiform, or saccular dilatation of intrahepatic bile ducts, also termed form fruste
-
Type V - Cystic, fusiform, or saccular dilatation of the intrahepatic bile ducts associated with a normal CBD; may be associated with hepatic fibrosis (referred to as Caroli disease)
Some authors describe a type VI, which consists of a choledochal cyst combined with dilatation of the cystic duct; this is very rare. [13]
Pathophysiology
Pathogenesis
The exact cause of choledochal cyst remains obscure. Because most of these cysts are diagnosed in infants and children, many authors believe that they are congenital. However, because approximately 20% are diagnosed in adults, including elderly patients, several theories have been postulated, as follows [3, 14] :
In 1969, Babbitt et al carefully analyzed the cholangiograms of patients with choledochal cysts and found many with an anomaly of the pancreaticobiliary junction. [25] In these patients, a small distal CBD entered the pancreatic duct at 2-3.5 cm from the ampulla of Vater, whereas the normal common channel is 5 mm or less. This may represent failure of normal separation of these two ducts during embryologic development. This proximal junction precludes the proper functioning of the sphincter of Oddi. The pressure in the pancreatic duct (30-50 cm H2O) exceeds the pressure in the CBD (25-30 cm H2O), favoring reflux of pancreatic secretions into the CBD.
Babbitt et al also noted a high amylase content in the fluid from the cysts. [25] The reflux of pancreatic juice could lead to weakness and dissolution of the wall of the CBD (see the image below).
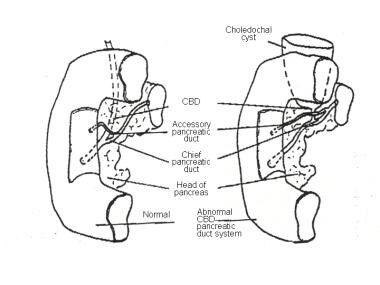 Anomalous pancreaticobiliary ductal system theory of choledochal cyst etiology. From Babbitt DP. [Congenital choledochal cysts: new etiological concept based on anomalous relationships of the common bile duct and pancreatic bulb]. Ann Radiol (Paris). 1969;12(3):231-40.
Anomalous pancreaticobiliary ductal system theory of choledochal cyst etiology. From Babbitt DP. [Congenital choledochal cysts: new etiological concept based on anomalous relationships of the common bile duct and pancreatic bulb]. Ann Radiol (Paris). 1969;12(3):231-40.
Experimental support for this concept was reported in 1974 by Kato et al, who anastomosed the main pancreatic duct to the gallbladder in dogs. [19] Within 9 days after the anastomosis, all the tested animals had varying degrees of dilatation of the CBD, with edematous changes of the CBD wall. They concluded that proteolytic enzymes were responsible for the damage.
In 1977, Spitz supported the concept of distal CBD obstruction as a cause of choledochal cyst when he demonstrated bile duct dilatation in lambs by means of ligation of the duct near the duodenum. [18] However, the same experiment failed to reproduce dilatation of the bile duct in mature sheep.
In 1981, Miyano et al established an experimental model of an anomalous choledochopancreatic ductal junction by creating a choledochopancreatic end-to-side ductal anastomosis in puppies. [26] They successfully reproduced the dilatation of the CBD in all experimental animals without exception.
In 1984, Todani et al conducted an analysis of endoscopic retrograde cholangiopancreatograms and other cholangiograms and confirmed this long common-channel anomaly. [27] The anomaly was found in most patients. Other authors have reported the same findings in their series. [28, 20, 21, 22, 29] Reflux of pancreatic enzymes into the CBD can happen early in life, even in fetal life, resulting in damage to the ductal wall. The distal portion of the CBD is most at risk, and with repeated irritation, it can become stenotic.
All of these theories are applicable to choledochal cyst type I, III, and IV anomalies, but they cannot be used to explain type II and V choledochal cysts in which the CBD is normal. Perhaps genetic factors play a role. [17, 30, 31] Despite this, the two most accepted theories are still (1) reflux of pancreatic enzymes into the CBD secondary to an anomalous pancreaticobiliary junction and (2) obstruction of the distal CBD.
Pathologic features
Grossly, the size of a type I choledochal cyst varies widely. [17, 28, 32, 33, 3, 34, 35, 36] The cysts contain a few hundred milliliters of bilious fluid that is rich in pancreatic enzymes. The cyst-wall thickness also varies, ranging from very thin to a few millimeters thick.
In type IV and V anomalies, intrahepatic cysts can be fusiform or saccular and are in continuity with the CBD. Dilatation of the proximal common duct is frequent, particularly just proximal to the long common channel. Sludge and stones are sometimes present within the cyst. [17, 30] The bile duct distal to the cyst is usually stenotic. The liver may have variable degrees of fibrosis or established cirrhosis with portal hypertension. Histologic studies of the wall of choledochal cysts show dense fibrous connective tissue with inflammation and ulceration of the mucosa and submucosal layers (see the image below).
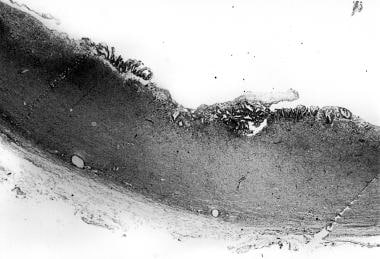 Photomicrograph shows the cyst wall, with inflammation and ulceration of the mucosa and submucosa.
Photomicrograph shows the cyst wall, with inflammation and ulceration of the mucosa and submucosa.
The inflammation is significantly less in younger patients than in older children in whom chronic inflammatory changes abound. [30, 29, 37, 36] With severe inflammation, only a relatively thin and fragmented lining, rather than the typical biliary mucosa, is observed lining the cyst. Intramucosal glandular structures are frequently observed; this suggests epithelial metaplasia secondary to repeated destruction and regrowth of the lining of the cyst. Inflammation has been noted to be more severe in intrahepatic cysts than in extrahepatic cysts.
Carcinoma arising in a choledochal cyst wall or remaining biliary tree after complete cyst excision is well recognized. [38] Malignancy is believed to be the result of chronic inflammation and metaplasia (see the image below). The typical malignancy is adenosquamous carcinoma or occasional cases of small cell carcinoma.

Epidemiology
Population prevalence estimates of choledochal cysts range from approximately one case in 13,000 people to one case in 2 million people. Cystic diseases of the bile duct are more common in Japan and Asia. [17] In an extensive review published in 1980, Yamaguchi et al reviewed 1433 cases from the literature; of these, 1204 (more than two thirds) were from Japan. [39]
In all reported series, the most frequent type of choledochal cyst is type I (see the image below and Anatomy). In types I and IV choledochal cysts (fusiform dilation of the CBD without or with dilated intrahepatic ducts, respectively), the female-to-male ratio is roughly 4:1. However, in types II (diverticulum of the CBD), III (choledochocele), and V (dilation of intrahepatic ducts only), the cysts occur with equal frequency in both sexes.
Choledochal cysts can occur in persons of any age. Two thirds of the cysts are diagnosed before the patient reaches the age of 10 years. [32, 33, 14] Approximately 20% of cysts are diagnosed in much older patients. [3, 22, 35] In rare cases, choledochal cysts have been detected at antenatal US as early as 15 weeks' gestation.
-
Todani classification of the 5 types of choledochal cysts.
-
Anomalous pancreaticobiliary ductal system theory of choledochal cyst etiology. From Babbitt DP. [Congenital choledochal cysts: new etiological concept based on anomalous relationships of the common bile duct and pancreatic bulb]. Ann Radiol (Paris). 1969;12(3):231-40.
-
Photomicrograph shows the cyst wall, with inflammation and ulceration of the mucosa and submucosa.
-
Media file shows the wall of the cyst, with inflammation and metaplasia.
-
Ultrasonogram shows a large unilocular cyst under the liver.
-
Magnetic resonance cholangiopancreatography shows dilated hepatic ducts and common bile duct (CBD) of a type IV cyst.
-
CT scan shows a large cyst with wall thickening.








