Overview
Injuries to the infant that result from mechanical forces (ie, compression, traction) during the birth process are categorized as birth trauma. Factors responsible for mechanical injury may coexist with hypoxic-ischemic insult; one may predispose the infant to the other. Lesions that are predominantly hypoxic in origin are not discussed in this article.
Significant birth injury accounts for fewer than 2% of neonatal deaths and stillbirths in the United States; it still occurs occasionally and unavoidably, with an average of 6-8 injuries per 1000 live births. [1] In general, larger infants are more susceptible to birth trauma. Higher rates are reported for infants who weigh more than 4500g.
Most birth traumas are self-limiting and have a favorable outcome. Nearly one half are potentially avoidable with recognition and anticipation of obstetric risk factors. Infant outcome is the product of multiple factors. Separating the effects of a hypoxic-ischemic insult from those of traumatic birth injury is difficult.
Risk factors for birth trauma include the following [2] :
-
Large-for-date infants, especially infants who weigh more than 4500 g
-
Instrumental deliveries, especially forceps (midcavity) or vacuum [3]
-
Vaginal breech delivery
-
Abnormal or excessive traction during delivery
Occasionally, injury may result from resuscitation. Recognition of trauma necessitates a careful physical and neurologic evaluation of the infant to establish whether additional injuries are present. Symmetry of structure and function should be assessed, the cranial nerves should be examined, and specifics such as individual joint range of motion and scalp/skull integrity should be evaluated.
Etiology
The birth process is a blend of compression, contractions, torques, and traction. When fetal size, presentation, or neurologic immaturity complicates this event, such intrapartum forces may lead to tissue damage, edema, hemorrhage, or fracture in the neonate. The use of obstetric instrumentation may further amplify the effects of such forces or may induce injury alone. Under certain conditions, cesarean delivery can be an acceptable alternative but does not guarantee an injury-free birth. Factors predisposing to injury include the following:
-
Prima gravida
-
Cephalopelvic disproportion, small maternal stature, maternal pelvic anomalies
-
Prolonged or rapid labor
-
Deep, transverse arrest of descent of presenting part of the fetus
-
Oligohydramnios
-
Abnormal presentation (breech)
-
Use of midcavity forceps or vacuum extraction
-
Versions and extractions
-
Very low birth weight infant or extreme prematurity
-
Fetal macrosomia
-
Large fetal head
-
Fetal anomalies
Prognosis
Birth injuries account for fewer than 2% of neonatal deaths. From 1970-1985, rates of infant mortality due to birth trauma fell from 64.2 to 7.5 deaths per 100,000 live births, a remarkable decline of 88%. This decrease reflects, in part, the technologic advancements that allow today's obstetrician to recognize birth trauma risk factors using ultrasonography and fetal monitoring prior to attempting vaginal delivery. The use of potentially injurious instrumentation, such as midforceps rotation and vacuum delivery, has also declined. The accepted alternative is a cesarean delivery. [4]
Injuries with a favorable long-term prognosis
Soft tissue injuries with a favorable long-term prognosis include the following (see the image below):
-
Abrasions
-
Erythema petechia
-
Ecchymosis
-
Lacerations
-
Subcutaneous fat necrosis
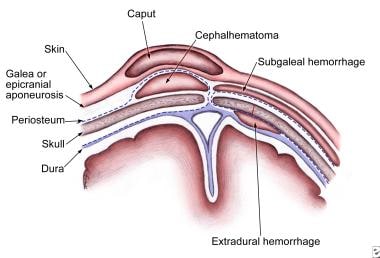 Birth Trauma. Location of injury in soft tissue planes on the scalp and head.
Birth Trauma. Location of injury in soft tissue planes on the scalp and head.

Skull injuries with a favorable long-term prognosis include the following:
-
Caput succedaneum
-
Cephalhematoma
-
Linear fractures
Facial injuries with a favorable long-term prognosis include the following:
-
Subconjunctival hemorrhage
-
Retinal hemorrhage
Musculoskeletal injuries with a favorable long-term prognosis include the following:
-
Clavicular fractures
-
Fractures of long bones
-
Sternocleidomastoid injury
Intra-abdominal injuries with a favorable long-term prognosis include the following:
-
Liver hematoma
-
Splenic hematoma
-
Adrenal hemorrhage
-
Renal hemorrhage
Peripheral nerve injuries with a favorable long-term prognosis include the following:
-
Facial palsy
-
Unilateral vocal cord paralysis
-
Radial nerve palsy
-
Lumbosacral plexus injury
Soft Tissue Injury
Soft tissue injury is associated with fetal monitoring, particularly with fetal scalp blood sampling for pH or fetal scalp electrode for fetal heart monitoring, which has a low incidence of hemorrhage, infection, or abscess at the site of sampling.
Cephalhematoma
Cephalhematoma is a subperiosteal collection of blood secondary to rupture of blood vessels between the skull and the periosteum; suture lines delineate its extent. Most commonly parietal, cephalhematoma may occasionally be observed over the occipital bone.
The extent of hemorrhage may be severe enough to cause anemia and hypotension, although this is uncommon. The resolving hematoma predisposes to hyperbilirubinemia. Rarely, cephalhematoma may be a focus of infection that leads to meningitis or osteomyelitis. [5] Linear skull fractures may underlie a cephalhematoma (5-20% of cephalhematomas). Resolution occurs over weeks, occasionally with residual calcification.
No laboratory studies are usually necessary. Skull radiography or computed tomography (CT) scanning is performed if neurologic symptoms are present. Usually, management solely consists of observation. Transfusion for anemia, hypovolemia, or both is necessary if blood accumulation is significant. Aspiration is not required for resolution and is likely to increase the risk of infection.
Hyperbilirubinemia occurs following the breakdown of the red blood cells (RBCs) within the hematoma. This type of hyperbilirubinemia occurs later than classic physiologic hyperbilirubinemia. The presence of a bleeding disorder should be considered. Skull radiography or CT scanning is also performed if a concomitant depressed skull fracture is a possibility.
Subgaleal hematoma
Subgaleal hematoma is bleeding in the potential space between the skull periosteum and the scalp galea aponeurosis. Ninety percent of cases result from a vacuum applied to the head at delivery. Subgaleal hematoma has a high frequency of occurrence of associated head trauma (40%), such as intracranial hemorrhage or skull fracture. [6] The occurrence of these features does not significantly correlate with the severity of subgaleal hemorrhage. [7]
The diagnosis is generally a clinical one, with a fluctuant, boggy mass developing over the scalp (especially over the occiput). The swelling develops gradually 12-72 hours after delivery, although it may be noted immediately after delivery in severe cases. The hematoma spreads across the whole calvaria; its growth is insidious, and subgaleal hematoma may not be recognized for hours.
Patients with subgaleal hematoma may present with hemorrhagic shock. The swelling may obscure the fontanelle and cross suture lines (distinguishing it from cephalhematoma). Watch for significant hyperbilirubinemia. In the absence of shock or intracranial injury, the long-term prognosis is generally good.
Laboratory studies consist of a hematocrit evaluation. Management consists of vigilant observation over days to detect progression and provide therapy for such problems as shock and anemia. Transfusion and phototherapy may be necessary. Investigation for coagulopathy may be indicated.
Caput succedaneum
Caput succedaneum is a serosanguineous, subcutaneous, extraperiosteal fluid collection with poorly defined margins. It is caused by the pressure of the presenting part against the dilating cervix and is associated with prolonged labor and instrument-assisted vaginal delivery. [8] Caput succedaneum extends across the midline and over suture lines and is associated with head molding. Caput succedaneum does not usually cause complications and usually resolves over the first few days. Management consists of observation only.
Abrasions and lacerations
Abrasions and lacerations sometimes may occur as scalpel cuts during cesarean delivery or during instrumental delivery (ie, vacuum, forceps). Infection remains a risk, but most of these lesions uneventfully heal.
Management consists of careful cleaning, application of antibiotic ointment, and observation. Bring edges together using Steri-Strips. Lacerations occasionally require suturing.
Subcutaneous fat necrosis
Subcutaneous fat necrosis is not usually detected at birth. Irregular, hard, nonpitting, subcutaneous plaques with overlying dusky, red-purple discoloration on the extremities, face, trunk, or buttocks may be caused by pressure during delivery. No treatment is necessary. Subcutaneous fat necrosis sometimes calcifies.
Brachial Plexus Injury
Peripheral nerve damage in the form of brachial plexus injury occurs most commonly in large babies, frequently with shoulder dystocia or breech delivery. Incidence for brachial plexus injury is 0.5-2 per 1000 live births. Most cases are Erb palsy; entire brachial plexus involvement occurs in 10% of cases.
Traumatic lesions associated with brachial plexus injury include the following:
-
Fractured clavicle (10%)
-
Fractured humerus (10%)
-
Subluxation of cervical spine (5%)
-
Cervical cord injury (5-10%)
-
Facial palsy (10-20%)
Erb palsy (C5-C6) is most common and is associated with lack of shoulder motion. The involved extremity lies adducted, prone, and internally rotated. Moro, biceps, and radial reflexes are absent on the affected side. The grasp reflex is usually present. Five percent of patients have an accompanying (ipsilateral) phrenic nerve paresis.
Klumpke paralysis (C7-8, T1) is rare and results in weakness of the intrinsic muscles of the hand; the grasp reflex is absent. If cervical sympathetic fibers of the first thoracic spinal nerve are involved, Horner syndrome is present.
A study by Iffy et al indicated that an approximately four-fold rise in the incidence of shoulder dystocia has occurred in the United States since the mid-20th century, with a review of 11 other countries revealing no comparable increase in most other nations. The investigators considered the rise in dystocia to be primarily related to a trend in the United States, starting in the 1980s, toward active management of the birthing process, in place of a more conservative approach. [9]
Prognosis
No uniformly accepted guidelines for determining prognosis are available. Narakas developed a classification system (types I-V) based on the severity and extent of the lesion, providing clues to the prognosis in the first 2 months of life. [10]
According to the collaborative perinatal study (59 infants), 88% of cases resolved in the first 4 months, 92% resolved by 12 months, and 93% resolved by 48 months. [11] In another study, which examined 28 patients with upper plexus involvement and 38 with total plexus palsy, 92% spontaneously recovered. [12]
Residual long-term deficits may include progressive bony deformities, muscle atrophy, joint contractures, possible impaired growth of the limb, weakness of the shoulder girdle, and/or Erb engram flexion of the elbow accompanied by adduction of shoulder.
In a study of nine neonates, Shen et al found that a rapid nonsedated volumetric Cube Proton Density magnetic resonance imaging (MRI) protocol performed at initial clinical presentation can accurately grade the severity of brachial plexus birth palsy injury and predict functional performance at age 6 months. [13] Proton Density MRI differentiated between preganglionic and postganglionic injuries. Shriners Radiological Score correlated better with functional performance at age 6 months than at the initial clinical examinations. [13]
Workup
Workup consists of radiographic studies of the shoulder and upper arm to rule out bony injury. The chest should be examined to rule out associated phrenic nerve injury. Electromyography (EMG) and nerve conduction studies are occasionally useful.
Fast spin-echo MRI can be used to evaluate plexus injuries noninvasively in a relatively short time, minimizing the need for general anesthesia. MRI can define meningoceles and may distinguish between intact nerve roots and pseudomeningoceles (indicative of complete avulsion).
Bauer et al found evidence that a new technique using three-dimensional volumetric proton density magnetic resonance imaging (MRI) without sedation can evaluate the severity of brachial plexus birth palsy (BPBP) injury earlier than serial clinical examinations.[ref16} In their study, infants were prospectively enrolled prior to 12 weeks of age, and 9 infants completed the MRI scan and clinical follow-up. Based upon their results, the investigators concluded that three-dimensional proton density MRI can evaluate spinal nerve roots in infants without the need for radiation, contrast agents, or sedation. [14]
Carefully performed, intrathecally enhanced CT myelography may show preganglionic disruption, pseudomeningoceles, and partial nerve root avulsion. CT myelography is more invasive and offers few advantages over MRI.
Immobilization, physical therapy, and surgery
Management consists of prevention of contractures. Immobilize the limb gently across the abdomen for the first week and then start passive range-of-motion exercises at all joints of the limb. Use supportive wrist splints.
The best results from surgical repair appear to be obtained in the first year of life. [15] Several investigators have recommended surgical exploration and grafting if no function is present in the upper roots at age 3 months, although the recommendation for early explorations is far from universal. [16]
Complications of brachial plexus exploration include infection, poor outcome, and burns from the operating microscope. Patients with root avulsion do not do well.
Palliative procedures involving tendon transfers have been of some use. Results from a study by Ruchelsman et al of 21 children who suffered brachial plexus birth injury indicated that patients who have no active wrist extension following the trauma can be successfully treated with a tendon transfer but that surgical outcomes tend to be worse in patients with global palsy. [17]
Latissimus dorsi and teres major transfers to the rotator cuff have been advocated for improved shoulder function in Erb palsy. One permanent and 3 transitory axillary nerve palsies have been reported from the procedure.
Cranial Nerve Injury
Cranial nerve and spinal cord injuries result from hyperextension, traction, and overstretching with simultaneous rotation; they may range from localized neurapraxia to complete nerve or cord transection.
Unilateral branches of the facial nerve and vagus nerve, in the form of recurrent laryngeal nerve, are most commonly involved in cranial nerve injuries and result in temporary or permanent paralysis.
Compression by the forceps blade has been implicated in some facial nerve injury, but most facial nerve palsy is unrelated to trauma from obstetric instrumentation (eg, forceps). The compression appears to occur as the head passes by the sacrum.
Physical findings for central nerve injuries are asymmetrical facies with crying. The mouth is drawn towards the normal side, wrinkles are deeper on the normal side, and movement of the forehead and eyelid is unaffected. The paralyzed side is smooth with a swollen appearance, the nasolabial fold is absent, and the corner of the mouth droops. No evidence of trauma is present on the face.
Physical findings for peripheral nerve injuries are asymmetrical facies with crying. Sometimes evidence of forceps marks is present. With peripheral nerve branch injury, the paralysis is limited to the forehead, eye, or mouth.
The differential diagnosis includes nuclear genesis (Möbius syndrome), congenital absence of the facial muscles, unilateral absence of the orbicularis oris muscle, and intracranial hemorrhage.
Management and recovery
Most infants begin to recover in the first week, but full resolution may take several months. Palsy that is due to trauma usually resolves or improves, whereas palsy that persists is often due to absence of the nerve.
Management consists of protecting the open eye with patches and synthetic tears (methylcellulose drops) every 4 hours. Consultation with a neurologist and a surgeon should be sought if no improvement is observed in 7-10 days.
Diaphragmatic paralysis
Diaphragmatic paralysis secondary to traumatic injury to the cervical nerve roots that supply the phrenic nerve can occur as an isolated finding or in association with brachial plexus injury. The clinical syndrome is variable. The course is biphasic; initially the infant experiences respiratory distress with tachypnea and blood gases suggestive of hypoventilation (ie, hypoxemia, hypercapnia, acidosis). Over the next several days, the infant may improve with oxygen and varying degrees of ventilatory support. Elevated hemidiaphragm may not be observed in the early stages. Approximately 80% of lesions involve the right side and about 10% are bilateral.
The diagnosis is established by ultrasonography or fluoroscopy of the chest, which reveals the elevated hemidiaphragm with paradoxic movement of the affected side with breathing.
Prognosis
The mortality rate for unilateral lesions is approximately 10-15%. Most patients recover in the first 6-12 months. An outcome for bilateral lesions is poorer. The mortality rate approaches 50%, and prolonged ventilatory support may be necessary.
Management consists of careful surveillance of respiratory status, and intervention, when appropriate, is critical.
Laryngeal Nerve Injury
Disturbance of laryngeal nerve function may affect swallowing and breathing. Laryngeal nerve injury appears to result from an intrauterine posture in which the head is rotated and flexed laterally. During delivery, similar head movement (when marked) may injure the laryngeal nerve, accounting for approximately 10% of cases of vocal cord paralysis attributed to birth trauma.
The infant presents with a hoarse cry or respiratory stridor, caused most often by unilateral laryngeal nerve paralysis. Swallowing may be affected if the superior branch is involved. Bilateral paralysis may be caused by trauma to both laryngeal nerves or, more commonly, by a central nervous system (CNS) injury, such as hypoxia or hemorrhage, that involves the brain stem. Patients with bilateral paralysis often present with severe respiratory distress or asphyxia.
Direct laryngoscopic examination is necessary to make the diagnosis and to distinguish vocal cord paralysis from other causes of respiratory distress and stridor in the newborn. Differentiate from other rare etiologies such as cardiovascular or CNS malformations or a mediastinal tumor.
Paralysis often resolves in 4-6 weeks, although recovery may take as long as 6-12 months in severe cases. Treatment is symptomatic. Once the neonate is stable, providing small, frequent feeds minimizes the risk of aspiration. Infants with bilateral involvement may require gavage feeding and tracheotomy.
Spinal Cord Injury
Spinal cord injury incurred during delivery results from excessive traction or rotation. Traction is more important in breech deliveries (the minority of cases), and torsion is more significant in vertex deliveries. The true incidence of spinal cord injuries is difficult to determine. The lower cervical and upper thoracic region for breech delivery and the upper and midcervical region for vertex delivery are the major sites of injury.
Major neuropathologic changes consist of acute lesions, which are hemorrhages, especially epidural lesions, intraspinal lesions, and edema. Hemorrhagic lesions are associated with varying degrees of stretching, laceration, and disruption or total transaction. Occasionally, the dura may be torn, and rarely, vertebral fractures or dislocations may be observed.
The clinical presentation is stillbirth or rapid neonatal death with failure to establish adequate respiratory function, especially in cases involving the upper cervical cord or lower brainstem. Severe respiratory failure may be obscured by mechanical ventilation and may cause ethical issues later. The infant may survive with weakness and hypotonia, and the true etiology may not be recognized. A neuromuscular disorder or transient hypoxic ischemic encephalopathy may be considered. Most infants later develop spasticity that may be mistaken for cerebral palsy.
The diagnosis is made using MRI or CT myelography. Little evidence indicates that laminectomy or decompression has anything to offer. A potential role for methylprednisolone is recognized. Supportive therapy is important.
Prevention is the most important aspect of medical care. Obstetric management of breech deliveries, instrumental deliveries, and pharmacologic augmentation of labor must be appropriate. Occasionally, injury may be sustained in utero.
Bone Injury
Fractures are most often observed following breech delivery, shoulder dystocia, or both in infants with excessive birth weights.
Clavicular fracture
The clavicle is the most frequently fractured bone in the neonate during birth; this is most often an unpredictable, unavoidable complication of normal birth. [18] Some correlation with birth weight, midforceps delivery, and shoulder dystocia is recognized. [19] The infant may present with pseudoparalysis. Examination may reveal crepitus, palpable bony irregularity, and sternocleidomastoid muscle spasm. Radiographic studies confirm the fracture.
Healing usually occurs in 7-10 days. In order to decrease pain, arm motion may be limited by pinning the infant's sleeve to the shirt. Assess other associated injury to the spine, brachial plexus, or humerus.
Long bone fracture
Loss of spontaneous arm or leg movement is an early sign of long bone fracture, followed by swelling and pain on passive movement. The obstetrician may feel or hear a snap at the time of delivery. Radiographic studies of the limb confirm the diagnosis and distinguish this condition from septic arthritis.
Femoral and humeral shaft fractures are treated with splinting. Closed reduction and casting is necessary only when displaced. Watch for evidence of radial nerve injury with humeral fracture. Callus formation occurs, and complete recovery is expected in 2-4 weeks. In 8-10 days, the callus formation is sufficient to discontinue immobilization. Orthopedic consultation is recommended.
Epiphysial displacement
Separation of the humeral or femoral epiphysis occurs through the hypertrophied layer of cartilage cells in the epiphysis. The diagnosis is clinically based on swelling around the shoulder, crepitus, and pain when the shoulder is moved. Motion is painful, and the arm lies limp by the side. Because the proximal humeral epiphysis is not ossified at birth, it is not visible on radiography. Callus appears in 8-10 days and is visible on radiography.
Management consists of immobilizing the arm for 8-10 days. Fracture of the distal epiphysis is more likely to have a significant residual deformity than is fracture of the proximal humeral epiphysis.
Intra-Abdominal Injury
Intra-abdominal injury is relatively uncommon and can sometimes be overlooked as a cause of death in the newborn. Hemorrhage is the most serious acute complication, and the liver is the most commonly damaged internal organ.
Signs and symptoms of intraperitoneal bleed
Bleeding may be fulminant or insidious, but patients ultimately present with circulatory collapse. Intra-abdominal bleeding should be considered for every infant who presents with shock, pallor, unexplained anemia, and abdominal distension. Overlying abdominal skin may have a bluish discoloration. Radiographic findings are not diagnostic but may suggest free peritoneal fluid. Paracentesis is the procedure of choice.
Hepatic rupture
The most common lesion is subcapsular hematoma, which increases to 4-5 cm before rupturing. Symptoms of shock may be delayed. Lacerations are less common; they are often caused by an abnormal pull on the peritoneal support ligaments or by the effect of excessive pressure by the costal margin. Infants with hepatomegaly may be at higher risk. Other predisposing factors include prematurity, postmaturity, coagulation disorders, and asphyxia. In cases associated with asphyxia, a vigorous resuscitative effort (often by unusual methods) is the culprit.
Splenic rupture is at least a fifth as common as liver laceration. Predisposing factors and mechanisms of injury are similar.
Rapid identification and stabilization of the infant are the keys to management, along with assessment of coagulation defect. Blood transfusion is the most urgent initial step. Persistent coagulopathy may be treated with fresh frozen plasma, the transfusion of platelets, and other measures.
Patients with hepatic rupture usually present immediately following birth, or the rupture becomes obvious within the first few hours or days after delivery.
-
Birth Trauma. Location of injury in soft tissue planes on the scalp and head.





