Background
Unroofed coronary sinus (UCS) is a rare atrial septal defect (ASD) that results in an abnormal communication between the coronary sinus and the left atrium. It is usually associated with other forms of congenital heart disease, typically heterotaxy syndromes. It is frequently associated with a persistent left superior vena cava (PLSVC), which is the most common anomaly of systemic venous drainage. [1]
History Of The Procedure
Symptomatology stems from left-to-right shunting through the communication between the UCS and the left atrium and from right-to-left shunting, if there is a PLSVC draining deoxygenated blood from the left upper body into the left atrium. Dyspnea, [2, 3] right-sided heart enlargement, [2, 3] and cyanosis [4] have been reported in adults and children. [5] The presence of a PLSVC also creates the risk of brain abscess and paradoxical embolization. [6]
When left untreated, this defect has been reported to cause right-sided heart failure. [7] Chauvin et al have hypothesized that failed ablation procedures in adults, such as the Cox maze, could be attributable to an undiagnosed coronary sinus ASD; in essence, the ASD provides a means of a residual conduction pathway. [8] If untreated, this defect may leave behind significant residual right-to-left shunting following surgical repair of other associated defects. [9]
Etiology
Coronary sinus ASDs account for less than 1% of all types of ASDs. [10] They are usually associated with other forms of congenital heart disease (eg, heterotaxy syndromes) or PLSVC. PLSVC occurs in 0.1-0.5% of the general population, with 8% draining into the left atrium. [5] UCS is seen in 75% of patients with a PLSVC that drains into the left atrium and is usually associated with other forms of congenital heart disease and heterotaxy syndromes. [1]
Pathophysiology
In normal fetal development, the paired anterior cardinal veins drain the upper body and extremities of the fetus and become connected by an oblique vessel. During the 8th week of embryological development, a communication forms between the veins (future innominate [brachiocephalic] vein). The distal end of the left anterior cardinal vein degenerates (forms the ligament of Marshall), and the remaining right anterior cardinal vein ultimately becomes the right superior vena cava (RSVC).
The distal end of the left anterior cardinal vein drains into the left horn of the sinus venosus (future coronary sinus) before it degenerates; this explains the drainage pattern of a PLSVC into the coronary sinus (see the image below). When a PLSVC drains into an UCS, obligate drainage to the left atrium results in the right-to-left shunt and cyanosis. [11] Failure of the distal left anterior cardinal vein to degenerate is possible with or without degeneration of the right cardinal veins. [1] A PLSVC can be the sole drainage of systemic venous blood in the upper extremities and the head or may occur in conjunction with a RSVC. With dual superior vena cavae (SVCs), a bridging innominate (brachiocephalic) vein is often not present.
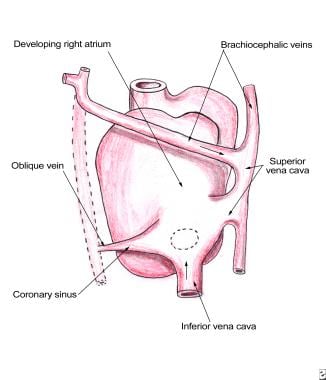 Pediatric Surgery for Unroofed Coronary Sinus. Embryologic remnant resulting in persistent left superior vena cava (PLSVC). The dotted line illustrates the degenerated left anterior cardinal vein. This posterior view illustrates how the left superior vena cava drains into the coronary sinus.
Pediatric Surgery for Unroofed Coronary Sinus. Embryologic remnant resulting in persistent left superior vena cava (PLSVC). The dotted line illustrates the degenerated left anterior cardinal vein. This posterior view illustrates how the left superior vena cava drains into the coronary sinus.
Presentation
Isolated UCS defects may not express any symptoms and can be found during the workup for a concomitant lesion in asymptomatic patients. [12, 13] When present, symptoms may range from mild cardiomegaly to overt congestive heart failure. The degree of volume overload is determined primarily by the size and degree of biatrial shunting. [2]
UCS should be suspected in a patient with a PLSVC and a history of brain abscesses or paradoxical emboli, in a patient with a left-to-right interatrial shunt with unexplained arterial oxygen desaturation, [13] or in the setting of a new-onset, poorly explained left-to-right shunt following cardiac surgery. [12] Coronary sinus ASDs have been reported to occur with several other congenital heart defects, such as endocardial cushion defects, [14] cor triatriatum, tetralogy of Fallot, [15] pulmonary atresia or stenosis, abnormal ventriculoarterial connection, [15] and anomalous pulmonary venous return. [10] It also has been reported in association with Noonan syndrome, which is characterized by ASDs with pulmonary stenosis and developmental delay. [16]
Indications
As in other ASDs, indications for surgical repair include complications from right-to-left shunting, right heart volume overload, paradoxical emboli, and brain abscesses. [6] UCS may be repaired when presenting with other cardiac lesions.
Relevant Anatomy
Coronary sinus type ASD is characterized by a communication between the coronary sinus and the left atrium. Several anatomic variations of this communication have been described, including partial fenestrations between the walls of the coronary sinus and left atrium to a complete atresia of the coronary sinus orifice. The "pure form" of this defect refers to total absence of the walls between the coronary sinus and left atrium, with a connection between a PLSVC and the left atrium in the presence of a heterotaxy syndrome. [5]
The PLSVC enters the pericardium anterior to the left pulmonary artery. It then runs posterior to enter the left atrium and drain through the coronary sinus to the right atrium. When the wall between the coronary sinus tube and left atrium fails to form, which is thought to be caused by the maldevelopment of the atriovenous fold, the systemic venous blood drains directly into the left atrium. This fenestration into the left atrium usually occurs between the left atrial appendage and the left upper pulmonary vein, as shown in the image below. [17] When this fold is missing, the defect is called a UCS or UCS-ASD.
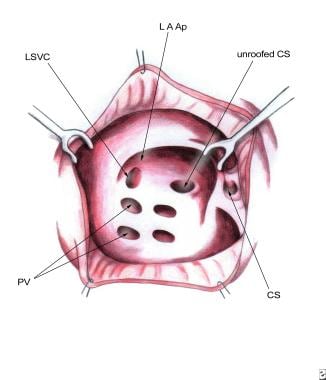 Pediatric Surgery for Unroofed Coronary Sinus. The fenestration is seen draining between the left atrial appendage and the pulmonary veins.
Pediatric Surgery for Unroofed Coronary Sinus. The fenestration is seen draining between the left atrial appendage and the pulmonary veins.
UCS has been classified morphologically into various types by Kouchoukos et al, [18] as follows:
-
Type I: Completely UCS with PLSVC
-
Type II: Completely UCS without PLSVC
-
Type III: Partially unroofed midportion of coronary sinus
-
Type IV: Partially unroofed terminal portion of coronary sinus
-
Unroofed sinus syndrome related to cor triatriatum and ASD
Contraindications
Surgery is contraindicated in the presence of major genetic abnormalities.
-
Pediatric Surgery for Unroofed Coronary Sinus. Embryologic remnant resulting in persistent left superior vena cava (PLSVC). The dotted line illustrates the degenerated left anterior cardinal vein. This posterior view illustrates how the left superior vena cava drains into the coronary sinus.
-
Pediatric Surgery for Unroofed Coronary Sinus. The fenestration is seen draining between the left atrial appendage and the pulmonary veins.
-
Pediatric Surgery for Unroofed Coronary Sinus. A venous cannula stent opens the coronary sinus while sutures are placed.
-
Pediatric Surgery for Unroofed Coronary Sinus. A pericardial patch is used to baffle the pulmonary veins directly toward the mitral valve. This approach allows unobstructed flow from the orifice of the left superior vena cava (LSVC) to drain to the right-sided atrium.





