Practice Essentials
Sjögren syndrome, which is rare in pediatric patients, is a slowly progressive inflammatory disorder that involves the exocrine glands. [1] Mikulicz and others recognized the findings of keratoconjunctivitis and xerostomia as an entity in the late 1800s. [2] In 1933, Sjögren recognized the association of this symptom complex with polyarthritis.
Subsequent studies showed that Sjögren syndrome may be a primary disorder or may be secondary to other autoimmune disorders, such as systemic lupus erythematosus (SLE), [3] rheumatoid arthritis, scleroderma, and biliary cirrhosis. Extraglandular manifestations may mimic these other autoimmune disorders. [1] The primary disorder is most common in women in the fourth and fifth decades of life. Sjögren syndrome may overlap with other pediatric autoimmune disorders and, less commonly, may present as a primary condition (see the images below). (See Etiology, Clinical, and Workup.) [4, 5]
The lower facial appearance of a 14-year-old adolescent girl with Sjögren syndrome is shown in the image below. She exhibits both parotid and submandibular gland enlargement and chapped lips.
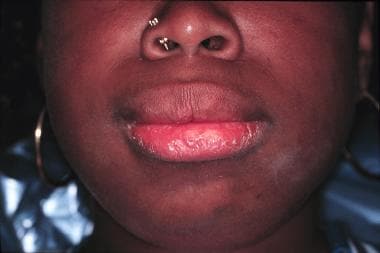 Lower facial appearance of a 14-year-old adolescent girl with Sjogren syndrome. She exhibits both parotid and submandibular gland enlargement and chapped lips.
Lower facial appearance of a 14-year-old adolescent girl with Sjogren syndrome. She exhibits both parotid and submandibular gland enlargement and chapped lips.
An intraoral view of a 14-year-old adolescent girl with Sjögren syndrome is shown below. Hyposalivation results in erythema of the mucosa, gingivitis, decalcification or white spot lesions of the teeth at the cervical margin, and dental caries with extensive restorations of the posterior teeth.
 Intraoral view of a 14-year-old adolescent girl with Sjogren syndrome. Hyposalivation results in erythema of the mucosa, gingivitis, decalcification or white spot lesions of the teeth at the cervical margin, and dental caries with extensive restorations of the posterior teeth.
Intraoral view of a 14-year-old adolescent girl with Sjogren syndrome. Hyposalivation results in erythema of the mucosa, gingivitis, decalcification or white spot lesions of the teeth at the cervical margin, and dental caries with extensive restorations of the posterior teeth.
The image below shows erythema of the labial mucosa with enlargement of the minor salivary glands and superficial mucoceles.
 Erythema of the labial mucosa with enlargement of the minor salivary glands and superficial mucoceles.
Erythema of the labial mucosa with enlargement of the minor salivary glands and superficial mucoceles.
The dorsal surface of the tongue demonstrates generalized atrophy of the filiform papillae, mild fissuring, and median rhomboid glossitis.
 The dorsal surface of the tongue demonstrates generalized atrophy of the filiform papillae, mild fissuring, and median rhomboid glossitis.
The dorsal surface of the tongue demonstrates generalized atrophy of the filiform papillae, mild fissuring, and median rhomboid glossitis.
The image below shows a 14-year-old adolescent girl with Sjögren syndrome with painful unilateral swelling of the knee and hyperpigmentation of the overlying skin.
 A 14-year-old adolescent girl with Sjogren syndrome with painful unilateral swelling of the knee and hyperpigmentation of the overlying skin.
A 14-year-old adolescent girl with Sjogren syndrome with painful unilateral swelling of the knee and hyperpigmentation of the overlying skin.
The systemic and extraglandular features of Sjögren syndrome define the choice and extent of anti-inflammatory and immunomodulatory therapy, clinical course and disease outcome. (See Prognosis, Treatment, and Medications.)
Overlapping symptoms consistent with SLE include neuropsychiatric manifestations, nephritis, and severe Raynaud phenomenon. [6] Severe systemic manifestations may also develop without overt features of other autoimmune disorders. [3]
Patient education
As Sjögren syndrome is a chronic disease, participation in a local or national support group may be beneficial. The Sjögren's Syndrome Foundation is an example of an organization that helps individuals cope with this disease. Additional resources can be found at the Lupus Foundation of America and the Arthritis Foundation. For patient education information, see the Arthritis Center, as well as Sjögren’s Syndrome.
Etiology
Multiple etiologic factors are likely involved in the pathogenesis of Sjögren syndrome. [1, 7] Lymphocytic infiltration in the glandular lobules is the characteristic abnormality in lacrimal or salivary gland biopsy findings. The disorder appears to be mediated by a complex cascade of immune events and is often characterized as an autoimmune exocrinopathy. [7, 8]
The predominant immune cells are activated memory CD4+ T cells that express alpha/beta T-cell receptors, suggesting a central role in the pathogenesis of this disorder. [7] Activated B cells are also found in the lesions, which may be responsible for the production of the autoantibodies to autoantigens Ro (SS-A) and La (SS-B). Anti-Ro (SS-A) is found in 40-45% of adult patients with Sjögren syndrome, and anti-La (SS-B) is found in 50% of these patients. The presence of anti-Ro (SS-A) and anti-La (SS-B) is associated with earlier onset, longer duration, and more extensive extraglandular manifestations of primary Sjögren syndrome.
Positivity in these antibodies appears to be higher in children, according to a systematic review of the literature (rheumatoid factor [RF], 66%; antinuclear antibody [ANA], 78%; SS-A, 74%; SS-B, 65%). [9, 10, 11] Because these autoantibodies are also observed in other autoimmune disorders, including SLE, further diagnostic tools must be used for a more definitive diagnosis.
Researchers have found a high prevalence of anti-Muscarinic-3 acetylcholine receptor autoantibodies in Japanese children with primary Sjögren syndrome. [12] These antibodies are postulated to be involved in defective glandular function and as anti-SSA and anti-SSBA, could be potentially useful as a diagnostic marker for primary Sjögren in children and adolescent.
Autoantibody production and evidence of a polyclonal gammopathy implicate B-cell dysfunction as a component of Sjögren syndrome pathogenesis. Increased levels of B-cell activating factor (BAFF) or B-lymphocyte stimulator (BLyS), which are essential for B-cell survival, can be found in patients with Sjögren syndrome. Thus, B-cell depletion therapies that include the anti-CD20 monoclonal antibody (rituximab) are being used in open-label studies. [13]
In situ evidence suggests that proinflammatory cytokines, interleukin (IL)-1, IL-6, and tumor necrosis factor (TNF)–alpha are produced in the salivary glands. These cytokines are found in the infiltrating lymphocytes and the epithelial cells. This suggests that the infiltrating lymphocytes (ie, predominantly CD4+ T cells) play a role in the perpetuation of an aberrant immune response. Specific IL-10 haplotypes are associated with early onset and vasculitic features of disease. IL-21 levels was noted to correlate positively with serum IgG and IL-21 expression is increased as more lymphocytes infiltrated in LSG among patients with primary SS. [14, 15] Additional cytokine and chemokine gene polymorphisms continue to be focus of several ongoing studies.
A higher incidence of Sjögren syndrome is found in family members of patients with the disease. The association of Sjögren syndrome with human leukocyte antigen (HLA)–B8, HLA-Dw3, HLA-DR3, and the DQA1*0501 allele supports the notion of genetic susceptibility. [16]
An active area of research involves genetic polymorphisms of cytokine genes, including IL10 and TNFA. [7] Associations with these polymorphisms might implicate inappropriate regulation of the immune response in Sjögren syndrome. Altered apoptotic mechanisms have also been implicated in the pathogenesis of Sjögren syndrome–related exocrinopathies. Exocrine gland tissue damage and chronic inflammation lead to fibrotic changes and impaired glandular function. The pathophysiology of extraglandular manifestations is thought to be due to similar immune mechanisms.
Epstein-Barr virus (EBV) replicates in the salivary glands during primary infection and remains latent in these organs. EBV deoxyribonucleic acid (DNA) is recovered from the salivary glands and saliva of patients with Sjögren syndrome. Its etiopathologic role cannot be proven. Human immunodeficiency virus (HIV), human T-cell leukemia-lymphoma virus type 1 (HTLV-1), and cytomegalovirus (CMV) are also being studied as possible inciting agents of the lymphoproliferation observed in the end organs.
Epidemiology
United States data
Overall, Sjögren syndrome is the second most common autoimmune disorder in adults, after rheumatoid arthritis. In the United States, between 500,000 and 2 million adults have this disease. [2]
Primary disease is rare in childhood, as only 145 cases of primary disease have been described in the international pediatric literature. [9] Five percent of adult patients report onset of symptoms before age 12 years. Clinical manifestations and classification schema differ in pediatric patients; therefore, this disorder may be underreported. Features of Sjögren syndrome are well described in pediatric patients who have other autoimmune disorders and oftentimes it is defined as an overlapping syndrome.
International data
Epidemiologic studies from different ethnic groups show prevalence rates similar to those in the United States.
Sex- and age-related demographics
The female-to-male ratio for Sjögren syndrome was 7:1 in one multicenter international pediatric cohort and 6:1 in a systematic review of the literature. [9, 10] In adults, the female-to-male ratio is approximately 9:1. [11]
In 2 studies, the mean age of diagnosis for primary juvenile Sjögren syndrome was 10 years. [9, 10] Although Sjögren syndrome has been recognized in patients of all ages, it primarily affects women in the fourth and fifth decades of life.
Prognosis
Patients with primary Sjögren syndrome usually have a good prognosis unless systemic and/or severe extraglandular manifestations develop. The prognosis of secondary Sjögren syndrome depends on the primary autoimmune disorder.
Although most adult patients have a mild and benign course, they often experience painful eye irritation, severe dental caries, and dyspareunia. Pediatric patients often do not have early sicca syndrome symptomatology but often have recurrent parotitis, which commonly is diagnosed as recurrent parotitis of childhood, another uncommon pediatric disorder with a bimodal age incidence of 2-5 and 10 years of age. Because of the insidious nature of these symptoms, patients often do not seek medical attention until more severe symptoms appear years later.
The time from disease onset until diagnosis is often 9 years in adults and perhaps as long as 3 years in pediatric patients. In a multicenter, retrospective review of 40 patients, few major complications were reported from time of onset (follow-up, 0-7.5 y). [10] According to another small report of pediatric patients with at least 3 years’ follow-up, minimal progression in disease status was reported. [17] Some pediatric patients may develop systemic features that involve the nervous system, kidney, and lungs. [10, 18, 19]
Lymphoproliferative disorders increase 40-fold in adult Sjögren syndrome. Although significant lymphoproliferation usually remains confined to the salivary and lacrimal glands, extraglandular lymphoproliferation (eg, lymphadenopathy, hepatosplenomegaly) sometimes resembles lymphoma (eg, pseudolymphoma) and may herald frank malignancies, including non-Hodgkin lymphoma, Waldenström macroglobulinemia, and B-cell lymphoma. Associations with lymphoproliferative diseases are not well described in pediatric populations.
-
Lower facial appearance of a 14-year-old adolescent girl with Sjogren syndrome. She exhibits both parotid and submandibular gland enlargement and chapped lips.
-
Intraoral view of a 14-year-old adolescent girl with Sjogren syndrome. Hyposalivation results in erythema of the mucosa, gingivitis, decalcification or white spot lesions of the teeth at the cervical margin, and dental caries with extensive restorations of the posterior teeth.
-
Erythema of the labial mucosa with enlargement of the minor salivary glands and superficial mucoceles.
-
The dorsal surface of the tongue demonstrates generalized atrophy of the filiform papillae, mild fissuring, and median rhomboid glossitis.
-
A 14-year-old adolescent girl with Sjogren syndrome with painful unilateral swelling of the knee and hyperpigmentation of the overlying skin.
-
The dorsal tongue demonstrates hyperplastic candidiasis with focal erosions and a brown hairy tongue. Ulcerated fissures are observed on the corners of the mouth that represent angular cheilitis.
-
Biopsy of the minor salivary glands of the lower lip may be useful in the diagnosis of Sjögren syndrome. A 1.5- to 2-cm incision of normal-appearing mucosa allows for the harvesting of 5 or more salivary gland lobules.
-
Low-power photomicrograph of a minor salivary gland lobule showing multiple lymphocytic foci that are replacing the acinar structures (hematoxylin-eosin, 40 X).
-
Intermediate-power photomicrograph demonstrating a chronic inflammatory aggregate of more than 50 lymphocytes and plasma cells with a periductal pattern. The inflammatory focus is adjacent to normal appearing acini (hematoxylin-eosin, 200 X).
-
High-power photomicrograph of the chronic inflammatory aggregate consists of lymphocytes and plasma cells around a ductal structure (hematoxylin-eosin, 400 X).