Background
Cardiac tumors were first described in the 18th century by Boneti; however, many believe the description by Albers in 1835 is the first authentic report. In 1936, the first successful removal of a neoplasm of the heart was performed. In 1952, angiography was first used for the diagnosis of heart tumors. In 1955, bypass was used for the first time to excise an intracavitary tumor. Cardiac tumors, whether primary or metastatic, are rare. [1, 2, 3]
The image below demonstrates a large tumor in the left ventricular cavity of the heart.
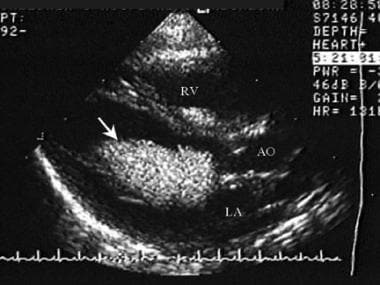 Pediatric Cardiac Tumors. Echocardiographic parasternal long-axis view showing a large mass within the left ventricular cavity invading or connected to the anterior mitral valve leaflet. AO=Aorta, RV=Right ventricle, LA=Left atrium, Arrow=Left ventricular mass.
Pediatric Cardiac Tumors. Echocardiographic parasternal long-axis view showing a large mass within the left ventricular cavity invading or connected to the anterior mitral valve leaflet. AO=Aorta, RV=Right ventricle, LA=Left atrium, Arrow=Left ventricular mass.
Benign neoplasms occur 3 times more often than malignant tumors. By far, the most common type of tumors reported in children and adolescents is rhabdomyoma (see image below), followed by fibroma, myxoma, and teratoma. [4] Sarcoma is the largest group of primary cardiac malignant neoplasms. Of these sarcomas, angiosarcomas are the most common histologic type and occur more frequently in males. These tumors directly seed blood, thus metastases are common and widespread. Signs and symptoms of these tumors at presentation are generalized, nonspecific, and mimic several other systemic diseases.
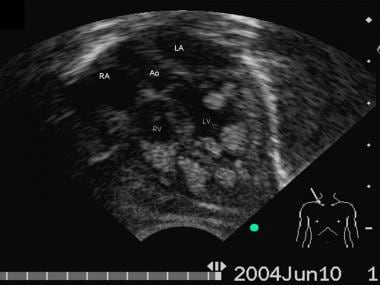 Pediatric Cardiac Tumors. Echocardiographic apical 5 chamber view of a 1 month old patient with several ventricular tumors filling the ventricular cavities in both sides. The patient was having seizures and diagnosed to have tuberous sclerosis. The tumor associated with this disease is rhabdomyoma (see text). RA= Right Atrium; Ao= Aorta; LA= Left Atrium; RV= Right Atrium; LV= Left Ventricle
Pediatric Cardiac Tumors. Echocardiographic apical 5 chamber view of a 1 month old patient with several ventricular tumors filling the ventricular cavities in both sides. The patient was having seizures and diagnosed to have tuberous sclerosis. The tumor associated with this disease is rhabdomyoma (see text). RA= Right Atrium; Ao= Aorta; LA= Left Atrium; RV= Right Atrium; LV= Left Ventricle
The clinical presentation of a patient with a cardiac tumor is determined more by the tumor's location than by its histologic type. Benign tumors, depending on their location, can present more symptoms than malignant tumors if they critically obstruct a valve or outflow tract. Consider the findings that are typical for each location.
Right-sided tumors may present with congestive heart failure (CHF) manifested by fatigue, edema, jugular venous distention, and ascites. Other symptoms include shortness of breath, syncope, and night sweats. Pericardial effusions may occur. Vena cava syndrome, pulmonary embolism, and restrictive cardiomyopathy are some of the complications.
Left atrial and left ventricular tumors can present various signs and symptoms that include, but are not restricted to, fever, chills, dizziness, dyspnea on exertion, cold sweats during exercise or at night, and nonproductive cough. Because tumors may embolize, they also can lead to seizures, transient ischemic attacks, and cerebrovascular and peripheral-vascular accidents. Based on their size and position, they may induce arrhythmias and interfere with ventricular compliance.
Benign tumors
Rhabdomyomas are hamartomas and are the most frequently found tumors in children as depicted in the images below. They are associated with tuberous sclerosis in about 50-80% of patients. Of patients with tuberous sclerosis, 50-60% have rhabdomyomas. These tumors are frequently multiple, involving ventricular free and septal walls, and have a yellowish-gray color. They vary from small to extremely large. They are rarely excised because they tend to regress over time; if patients are asymptomatic, only observation is warranted. Surgical removal is indicated when they present with obstruction leading to cardiac compromise or intractable arrhythmias. [5, 6]
Pediatric Cardiac Tumors. Echocardiographic apical 5 chamber view of a 1 month old patient with several ventricular tumors filling the ventricular cavities in both sides. The patient was having seizures and diagnosed to have tuberous sclerosis. The tumor associated with this disease is rhabdomyoma (see text). RA= Right Atrium; Ao= Aorta; LA= Left Atrium; RV= Right Atrium; LV= Left Ventricle
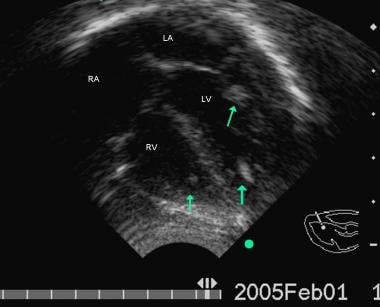 Pediatric Cardiac Tumors. Follow-up echocardiographic 4 chamber view from the same patient as shown in the image above. This echocardiogram was done 8 months after the previous view. Note that the tumors have changed in size and some of them have regressed totally, especially in the right ventricle. The arrows show the remaining areas of tumors seen in both ventricles.
Pediatric Cardiac Tumors. Follow-up echocardiographic 4 chamber view from the same patient as shown in the image above. This echocardiogram was done 8 months after the previous view. Note that the tumors have changed in size and some of them have regressed totally, especially in the right ventricle. The arrows show the remaining areas of tumors seen in both ventricles.
Fibromas, usually single and large, are most commonly found in the left ventricular free wall and rarely involve the septal wall. As many as 40% of fibromas are diagnosed in infants younger than 1 year. These tend to be firm nonencapsulated tumors derived from fibroblasts.
Myxomas are usually seen in adults. They are rarely seen in children, accounting for only 9-15% of all cardiac tumors from birth to adolescence. They are often found attached to the atrial septum and mitral valve apparatus in the left atrium (>85%). Myxomas can appear sporadically or as part of the syndrome myxoma or Carney syndrome, which includes endocrine neoplasms, tumors in other organs, and skin with spotty hyperpigmentation. This type of familial cardiac myxoma accounts for less than 10% of the myxomas appearing in the heart. They have an autosomal dominant transmission and most commonly appear in females. Patients with syndrome myxoma tend to be younger than those with sporadic myxomas. Myxomas may embolize; this may be their first clinical presentation. Peripheral embolization is reported to occur in as many as 70% of patients with myxomas and may even occur in utero.
Teratomas are single, encapsulated, grayish-tan tumors that appear most often in the pericardium. Teratomas develop in the right atrium, right ventricle, and septum of the heart. They are large basal tumors that, in newborns, may be larger than the patient's own heart.
Angiomas are a benign proliferation of endothelial cells, also known as vascular tumors. They can occur in any part of the heart (with a preference for right-sided chambers) and can form blood vessels (hemangiomas) or lymph vessels (lymphangiomas). These vascular vessels communicate between themselves within the myocardium. They can infiltrate the intraventricular septum near the conduction system where they may cause heart block. Hemangiomas are red, hemorrhagic, sessile, or polypoid subendocardial nodules that vary from small to large and occasionally have been associated with hemorrhagic cardiac tamponade.
Other types of tumors that have been less frequently reported in children include lipomas, papillary tumors, accessory cardiac cushion tissue, leiomyomas, mesotheliomas, fibroelastomas, fibroelastic papillomas, and benign cystic tumors.
Malignant tumors
Sarcomas originate from mesenchyme and, therefore, display a wide variety of morphologic types. These tumors are rare in children, with angiosarcoma being the most common type of sarcoma for all ages.
Cardiac angiosarcomas are characteristically lobulated variegated masses that are necrotic or hemorrhagic and are composed of anastomosing vascular channels lined by malignant cells that may contain areas of spindle cells. They tend to be aggressive malignancies, either infiltrative or polypoid, with most arising from the right atrium. Metastases are common and, based on autopsy studies, occur in as many as 88% of patients with malignant tumors.
Rhabdomyosarcomas grow invasively, metastasize, and can recur. These tumors are rare and are more common in children because they may arise from embryonic cell rests in the septum.
Fibrosarcomas, often involving more than one chamber of the heart, contain areas of hemorrhage and necrosis.
Other malignant neoplasms
Other reported malignant cardiac tumors are lymphomas, histiocytoma, leiomyosarcomas, choriocarcinoma, liposarcoma, and osteogenic sarcomas.
Etiology
Mutations in the gene protein kinase A (PKA) were identified in patients with Carney complex and myxomas. [8] A mutation of the gene that causes neurofibromatosis is present in patients who have neurofibromatosis and cardiac tumors. Whether or not this means cardiac tumors are directly related to neurofibromatosis is uncertain, although a relationship is likely.
Studies have described the relationship between angiogenesis and tumor growth. [9] Cardiac myxomas produce vascular endothelial growth factor, probably inducing angiogenesis for tumor growth. Neoangiogenesis is involved in the development of masses in the heart, benign or malignant. This knowledge is important for the possible creation of adjuvant therapies for inhibition of the tumor.
Epidemiology
United States data
Primary cardiac tumors are rare, with a frequency of 0.0017-0.28% based on autopsies. About 75% of them are benign and 25% are malignant. Secondary (metastatic) tumors are 10-40 times more frequent. Lam et al reviewed 12,485 autopsies and found only 7 cases of primary neoplasm of the heart versus 154 cases of secondary heart tumors. [7]
Rhabdomyomas are the most common tumor in children, with approximately 75% diagnosed in children younger than 1 year. Of these tumors, 50-80% are associated with tuberous sclerosis. Fibromas are the second most common tumor in children, with most (40%) diagnosed in children younger than 1 year. Myxomas are seen in 9-15% of patients with cardiac tumors, are the most common primary cardiac neoplasms in all ages, and comprise 50-60% of all heart tumors. The true incidence of teratomas is not known; however, 50% are diagnosed in newborns and 66% in children younger than 1 year. Sarcomas comprise 25% of all cardiac tumors; the most frequent tumor found is angiosarcoma.
Race-, sex-, and age-related demographics
No racial predilection is observed.
Myxomas are more common in females, especially in patients with syndrome myxoma or Carney syndrome. Angiosarcomas have a 2:1 male-to-female ratio. Rhabdomyomas, fibromas, teratomas, other sarcomas, and malignant tumors do not have any sex predilection.
No specific age predilection is noted; however, rhabdomyomas, fibromas, teratomas, and rhabdomyosarcomas are more commonly seen in children and adolescents than in adults. Myxomas comprise 50-60% of all benign tumors of the heart and are found mainly in adults.
Prognosis
Studies provide a wide spectrum of morbidity and mortality statistics.
Survival rates depend on the type of tumor, such as the following:
-
Benign tumors have a good prognosis unless they are associated with severe obstruction or intractable arrhythmias, which have a slightly higher risk of mortality.
-
For primary cardiac malignant tumors, the prognosis is invariably poor.
-
Metastatic neoplasms to the heart are more common than primary cardiac neoplasms; the prognosis is dependent on the histologic type of tumor, and survival rates are based on original pathology.
-
Certain tumors are known to recur even after resection.
-
Most children with cardiac tumors have an excellent prognosis and do not need any intervention.
Complications
Complications include arrhythmia, congestive heart failure (CHF), thromboembolism, decrease in ventricular function, and seeding during surgical removal (metastasis).
For complications related to specific types of cardiac tumors, see Background.
-
Pediatric Cardiac Tumors. Echocardiographic parasternal long-axis view showing a large mass within the left ventricular cavity invading or connected to the anterior mitral valve leaflet. AO=Aorta, RV=Right ventricle, LA=Left atrium, Arrow=Left ventricular mass.
-
Pediatric Cardiac Tumors. Echocardiographic subcostal view of a patient with a large mass within the left ventricular cavity invading or connected to the anterior mitral valve leaflet. Mass within the left ventricle fills most of the ventricular cavity. LA=Left atrium, RA=Right atrium, RV=Right ventricle, Arrow=Left ventricular mass.
-
Pediatric Cardiac Tumors. Echocardiographic parasternal long-axis view demonstrating a rounded mass in the area of the right ventricular outflow tract. Mass was not causing any outflow obstruction. RV=Right ventricle, LV= Left ventricle, AO=Aorta, Arrow=Right ventricular mass.
-
Pediatric Cardiac Tumors. Echocardiographic apical 5 chamber view of a 1 month old patient with several ventricular tumors filling the ventricular cavities in both sides. The patient was having seizures and diagnosed to have tuberous sclerosis. The tumor associated with this disease is rhabdomyoma (see text). RA= Right Atrium; Ao= Aorta; LA= Left Atrium; RV= Right Atrium; LV= Left Ventricle
-
Pediatric Cardiac Tumors. Follow-up echocardiographic 4 chamber view from the same patient as shown in the image above. This echocardiogram was done 8 months after the previous view. Note that the tumors have changed in size and some of them have regressed totally, especially in the right ventricle. The arrows show the remaining areas of tumors seen in both ventricles.





