Practice Essentials
Blastomycosis is a systemic pyogranulomatous infection usually caused by the inhalation of (spores) conidia of Blastomyces dermatitidis. Clinical presentations vary widely, ranging from an asymptomatic, self-limited pulmonary infection to acute respiratory distress syndrome (ARDS), a life-threatening disease. [1]
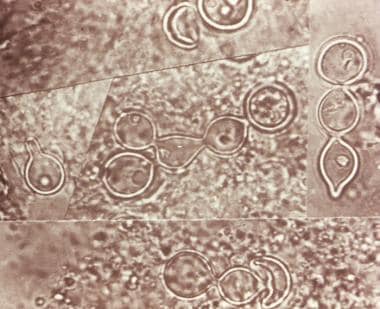 Composite photomicrograph of a tissue specimen from a patient with blastomycosis infection shows an abundance of large budding cells that had been configured in chains. Courtesy of CDC/Dr. Lucille K. George.
Composite photomicrograph of a tissue specimen from a patient with blastomycosis infection shows an abundance of large budding cells that had been configured in chains. Courtesy of CDC/Dr. Lucille K. George.
Signs and symptoms
Blastomycosis is usually localized to the lungs and may present with:
-
A self-limited flulike illness with fever, chills, myalgia, headache, and a nonproductive cough
-
An acute illness resembling bacterial pneumonia, with high fever, chills, a productive cough, and pleuritic chest pain; mucopurulent or purulent sputum
-
Chronic illness, with low-grade fever, a productive cough, fatigue, night sweats, and weight loss
-
Rapidly progressive, and severe disease (eg, multilobar pneumonia or ARDS), with fever, shortness of breath, tachypnea, hypoxemia and, finally, hemodynamic collapse
Extrapulmonary manifestations are present in 25-40% of patients, who may present with:
-
Cutaneous lesions - Usually either verrucous or ulcerative and may be asymptomatic
-
Osteoarticular lesions - Cause bone or joint pain; possible soft-tissue swelling; possible involvement of any bone, but the vertebrae and pelvis are common sites
-
Genitourinary manifestations including prostatitis and epididymitis - May be asymptomatic or may cause pain on urination
-
Other sites - B dermatitidis has been reported to involve almost all organs, including the eye, liver, spleen, breast, thyroid, and adrenal gland.
-
Central nervous system involvement - Intracranial or epidural abscesses and meningitis
See Presentation for more detail.
Diagnosis
Culture and cytopathology are the gold standard for the diagnosis of blastomycosis. The fastest way to diagnose blastomycosis is direct identification of the broad based budding yeast forms under microscopy. Identification from culture may not be evident for 2 to 4 weeks, and it often requires invasive procedures such as bronchoscopy or tissue biopsy to obtain specimens. [1]
More recently, molecular DNA probes have been developed to facilitate the rapid identification of B dermatitidis from clinical specimens. A commercially available chemiluminescent DNA probe assay (AccuProbe) is commonly used and produces results from culture within hours once there is adequate growth. [2]
In addition, tests targeting virulence factors BAD1 and DRK1 through real-time polymerase chain reaction (RT-PCR) and serologic antibody-based assays have been developed but are as yet not commercially available. [3, 4, 5]
Chest imaging findings are nonspecific and may range from scattered centrilobular nodules to areas of dense consolidation. Computed tomography (CT) scanning is not always necessary, but it can provide better definition of the character and distribution of abnormalities observed on a chest radiograph.
See Workup for more detail.
Management
Antifungal treatment is as follows:
-
Patients with mild to moderate pulmonary disease - Oral azole (eg, itraconazole)
-
Patients with moderate-to-severe disseminated disease or immune compromise: Initially, amphotericin B with step-down to an oral azole after clinical improvement
-
Patients with central nervous system (CNS) disease as well as pregnant women: Always be treat initially with amphotericin B
See Treatment and Medication for more detail.
Background
Oral azoles, usually itraconazole or amphotericin B, are first-line treatment for blastomycosis depending on the severity of the disease, its clinical form, and the host's immune status. In general, mild to moderate disease is typically treated with oral itraconazole—except in pregnant women and those with CNS disease, all of whom should always receive amphotericin B. Patients with moderately severe to severe disseminated disease should receive amphotericin B followed by a long-term oral azole when they clinically improve. [6]
Blastomycosis requires prolonged treatment. Patients with mild to moderate disseminated blastomycosis without central nervous system involvement should be treated for 6 months. In patients with bone involvement, the treatment period should be extended to 12 months. Individuals with severe disease occasionally require even longer treatment. See Treatment and Medication.
Pathophysiology
Blastomycosis is a systemic pyogranulomatous infection caused by the inhalation of conidia (spores) of B dermatitidis, the asexual (imperfect) form of Ajellomyces dermatitidis, a dimorphic fungus. The mycelial form grows as a fluffy white mold at 25°C (77°F) and a brown folded yeast at 37°C (98.6°F). The conidia are round, ranging from 2 to 10 μm in diameter, and become aerosolized when the fungus in the mycelia phase in the soil is disturbed. These can be inhaled, passing into the lower respiratory tract and resulting in pulmonary infection.
The inhaled conidia are phagocytized by bronchopulmonary mononuclear cells. The organism’s susceptibility to phagocytosis and killing by neutrophils, monocytes, and alveolar macrophages explain why some individuals remain asymptomatic despite exposure to environments that would cause clinical infection in others. At 37°C (98.6°F), B dermatitidis converts from the mycelial form to the yeast form.
This transformation provides a survival advantage to the infecting fungus, as the yeast form is larger, at 8-10 μm in diameter, and possesses a thick cell wall that provides greater resistance to phagocytosis and killing. The histidine kinase DRK1 regulates dimorphism from mold to yeast and virulence gene expression in B dermatitidis. DRK1 knockout strain grown at 37°C (98.6°F) is locked in the mold morphology. [7] Another virulence factor is BAD-1, an immune-modulating glycoprotein that is expressed on the cell surface and released into the extracellular matrix. [8] BAD-1 facilitates the binding of B dermatitidis to macrophages. The yeast forms multiply and may disseminate through the blood and lymphatics to other organs. The evoked pyogranulomatous inflammatory response is a distinctive feature of blastomycosis characterized by an initial influx of neutrophils, followed by macrophage and granuloma formation.
Blastomycosis may be asymptomatic in nearly 50% of infected persons. In the remainder, the median incubation period from inhalation of the fungus to manifestations of symptoms is 45 days (range: 21-106 days). Symptoms of blastomycosis are similar to influenza, with most patients presenting with cough, fever, sputum production, chest pain, and dyspnea. Cellular immunity is a major protective factor in preventing progressive disease secondary to B dermatitidis.
The lungs are the usual point of entry. In one study, pulmonary involvement was present in 91% of all cases. [9] Pulmonary symptoms range from acute and chronic pneumonias to acute respiratory distress syndrome (ARDS). Evidence of dissemination to other organs may be present.
Rarely, an extrapulmonary site (eg, skin, bone) may be the only presenting clinical manifestation.
In earlier reported case series, extrapulmonary involvement was noted in 50% of chronic blastomycosis cases. However, in present times, with earlier recognition and effective treatment, the extrapulmonary manifestations are seen in only about 20% of cases. Extrapulmonary dissemination occurs more commonly in patients with chronic pulmonary illness or immunocompromise.
Skin is the most common site of extrapulmonary blastomycosis and is involved in about 20% of cases. Other areas affected, and the approximate frequency of such involvement, are as follows [9] :
-
Bone - 5%
-
Prostate and other genitourinary organs - 2%
-
Meninges and brain - 1%
-
Other (lymph nodes, adrenal, eye, liver, spleen, trachea, breast, and thyroid) - 3%
Reactivation of blastomycosis may occur after a pulmonary infection that resolved, with or without treatment. An extrapulmonary site (eg, skin, bone, brain) is rarely a site of reactivation.
Etiology
Relatively recent advances in genotyping of Blastomyces by microsatellite typing and ITS2 sequencing have demonstrated that there are two unique clades, or species, of Blastomyces: B dermatitidis infection is more prevalent in patients with comorbidities and more likely to cause disseminated infection, and B gilchristii is more likely to cause isolated pulmonary disease. In a retropective review of children with blastomycosis confirmed by culture or cytopathology, the majority of the children had isolated pulmonary disease with systemic findings. [10] Those with extrapulmonary disease were less likely to have systemic symptoms or additional laboratory evidence of infection, which made delays in diagnosis more common. More than 90% of the pediatric cases were caused by B gilchristii. [11]
B dermatitidis is the asexual (imperfect) form of Ajellomyces dermatitidis, which is a thermal dimorphic fungus. The mycelial form grows as a fluffy white mold at 25°C (77°F) and a brown folded yeast at 37°C (98.6°F) body temperature. The fungus is usually isolated in the soil in its mycelial form in wet earth that has been enriched with animal droppings, rotting wood, and other decaying vegetable matter.
The conidia are round, ranging from 2 to 10 μm in diameter, and become aerosolized when the fungus in the mycelia phase is disturbed. The conidia are inhaled, passing into the lower respiratory tract and resulting in pulmonary infection. In infected tissue specimens, B dermatitidis appears as a characteristic thick-walled yeast, 8-10 μm in diameter, which provides greater resistance to phagocytosis and killing.
As dogs are infected with blastomycosis in a similar way and often in the same place as humans, an early clue to the diagnosis in humans is a history of a fungal infection in a pet dog. Blastomycosis is not transferred from animals to humans other than from bite wounds. [12] This condition has also been reported in other animals, including horses, cows, cats, bats, foxes, and lions.
Epidemiology
United States statistics
Blastomycosis can be endemic or sporadic. Most cases of blastomycosis occur in the United States and Canada, although occasional cases have been reported in Central and South America, Africa, the United Kingdom, India, and the Middle East. [13] The disease is endemic in the central and southeastern parts of the United States, near the Mississippi River, Ohio River, and Great Lakes. Thus, Arkansas, Kentucky, Mississippi, North Carolina, Tennessee, Louisiana, Illinois, and Wisconsin are commonly affected. [14] However, blastomycosis is reportable only in five states: Arkansas, Louisiana, Michigan, Minnesota, and Wisconsin. [15]
The true incidence and prevalence of blastomycosis are unknown, because there are no reliable antigen markers for skin testing. Its incidence in Northern Ontario has been reported as 117.2 cases per 100,000 population, the highest incidence in North America. [16] Based on confirmed cases, the annual US incidence is 1-2 cases per 100,000 people in Arkansas, Louisiana, Michigan, Minnesota, and Wisconsin. [6] Wisconsin may have the highest incidence of blastomycosis of any state, with yearly rates ranging from 10 to 40 cases per 100,000 persons in some northern counties, [17] and 2.9 hospitalizations per 100,000 person-years. [18] 2012 data from Illinois and Wisconsin found an annual incidence of 0.4-2.6 cases per 100,000 population; in contrast, 2007-2017 data from New York revealed an average annual incidence of 0.1-0.2 cases per 100,000. [15]
There were 1,216 blastomycosis-related deaths in the United States during 1990–2010. [19] Among those 1,216 deaths, blastomycosis was reported as the underlying cause of death for 741 (60.9%) and as a contributing cause of death for 475 (39.1%). The overall age-adjusted mortality rate for the period was 0.21 per 1 million person-years. [19]
Significant construction, such as interstate road expansion, can release Blastomyces spores from the soil. [20] One such urban outbreak comprised 34 confirmed cases of blastomycosis in Indianapolis from 2005 to 2008, which coincided with a period of major highway construction in the same area. [20] Residence near rivers and waterways is also associated with an increased risk of blastomycosis, particularly major freshwater drainage basins such as those of the Nelson River, St Lawrence River and northeast Atlantic Ocean Seaboard, Mississippi River System, and Gulf of Mexico Seaboard and southeast Atlantic Ocean Seaboard. [21] In Vilas County, north-central Wisconsin, 73 patients with laboratory-confirmed blastomycosis were identified over an 11-year period, in which 82% of these patients lived or had visited within 500 m of rivers or associated waterways. [22]
As noted under Etiology, canine blastomycosis can be an early warning sign for concomitant blastomycosis in humans. One case series of five households in which six patients were diagnosed with blastomycosis, one or more pet dogs were diagnosed with blastomycosis an average of 6 months before the patients themselves became symptomatic. [12]
International statistics
Blastomycosis can be seen outside of the United States. Internationally, most reported cases stem from Canada (Ontario, Manitoba) and Africa. Most African cases originate from South Africa [23] and Zimbabwe, [24] although cases have also been seen in Nigeria [25] and Tunisia. [26, 27] The disease is often mistaken for pulmonary tuberculosis or malignancy, and only after lack of response to standard treatment is the diagnosis made. [24, 25, 28] Cases have also been reported from disparate regions, including China, [16] Mexico, South America, the Middle East, and India. [13]
Because of the erroneous belief that the disease is limited to the United States, blastomycosis is often referred to as North American blastomycosis, which is an obsolete term. The term European blastomycosis is a confusing synonym of cryptococcosis, a systemic infection caused by the yeastlike fungus Cryptococcus neoformans. Likewise, South American blastomycosis (ie, Brazilian blastomycosis) is an older name for paracoccidioidomycosis, a chronic, often fatal, mycosis caused by a large dimorphic fungus, Paracoccidioides brasiliensis.
Racial, sexual, and age-related differences in incidence
Most studies of blastomycosis have shown no racial disparity in susceptibility. Rather, the distribution tends to mirror the ethnic and racial makeup of the area affected. However, in a few case series, certain races show a higher incidence of the disease. Some examples include an outbreak in Wisconsin, where 20 of the 55 patients affected were Hmong, [29] and an analysis of Missouri cases in which 57% of those affected were black although black individuals account for only 13% of the population. [30] One possible explanation for these findings is that these groups have greater exposure to environments containing wet soil or organic matter where B dermatitidis thrives.
Blastomycosis has been reported to occur more frequently in males, possibly due to greater occupational and recreational exposure. Men are more likely to participate in activities associated with B dermatitidis, such as fishing, hunting, and camping. In Wisconsin from 1986 to 1995, 60% of cases were in males. [31] However, analysis of outbreak cases from a common source and more recent reports do not indicate a significant sex difference. [32] Moreoever, historically, epidemiologic reports were skewed due to the collection of data from Veterans Administration (VA) hospitals nationwide, which predominantly serve male patients. [33]
The mean age at diagnosis is approximately 45 years, with most patients aged 30-69 years. However, persons of any age can acquire the disease, including infants and very elderly persons. [34]
The disease is rare in children and adolescents. A retrospective study at a children's hospital in Arkansas identified only 10 patients diagnosed with the disease between 1983 and 1995. [35] In past reviews, however, about 2-10% of patients reported were younger than 15 years. In children, both sexes are equally susceptible.
Prognosis
Immunocompetent patients with blastomycosis generally do not experience complications and can expect a full recovery. Relapse or recurrence of blastomycosis is rare, and it varies by the therapeutic agent, treatment length, and patient's immune capacity. Successful blastomycosis treatment is achieved in 80-95% of cases. [10] In contrast, immunocompromised patients with blastomycosis have a poor prognosis.
Cellular immunity is the fundamental host defense against B dermatitidis. Loss or compromise in T-lymphocyte function—for example, in human immunodeficiency virus infection / acquired immunodeficiency syndrome (HIV/AIDs) or with immune suppression after solid organ transplant, can predispose to severe disseminated disease or cavitary lung disease, and it often involves the central nervous system (CNS). [36, 37, 38]
Complications
Potential complications include progressive pulmonary disease and extrapulmonary dissemination. Risk of dissemination is increased in immunocompromised individuals. Severe pulmonary disease complicated by cavitary lesions and acute respiratory distress syndrome (ARDS) occurs in approximately 20% of compromised hosts. [39] CNS disease appears to be 3-5 times more common in immunocompromised patients than in immunocompetent hosts. Meningitis or mass lesions has/have been reported to occur in approximately 40% of adult patients with AIDS.
Extrapulmonary disease, frequently to the skin, bones, genitourinary system, and CNS, can occur in 25-40% of patients with blastomycosis. The skin is the second-most common site of involvement after the lungs, and cutaneous findings range from the characteristic verrucous lesions to friable ulcerative lesions. Complications include abscesses and nodules, and extensive cutaneous lesions may undergo central healing with scarring and contracture.
Osteomyelitis occurs in approximately 25% of extrapulmonary cases, [14] usually concomitantly with pulmonary blastomycosis. The infection can spread into nearby joints, leading to septic arthritis, or contiguous spread from the vertebral bodies can cause psoas abscesses.
Patient Education
Although immunocompromised patients (including those with human immunodeficiency virus infection / acquired immunodeficiency syndrome [HIV/AIDS]) living in or visiting blastomycosis-endemic areas cannot completely avoid exposure to B dermatitidis, they should be counseled about reducing the risk of acquiring blastomycosis by avoidance of occupational and recreational activities known to be associated with increased risk (eg, wooded areas along waterways).
-
Cutaneous blastomycosis.
-
Lateral chest radiograph reveals the ill-defined lingular opacity and an absence of pleural effusions.
-
Composite photomicrograph of a tissue specimen from a patient with blastomycosis infection shows an abundance of large budding cells that had been configured in chains. Courtesy of CDC/Dr. Lucille K. George.








