Background
Because hypoplastic left heart syndrome (eg, aortic atresia with mitral hypoplasia), pulmonary atresia with intact ventricular septum, and tricuspid atresia are discussed in other articles, this article considers the term "single ventricle" to apply to a double-inlet ventricle or common-inlet ventricle, two (or more, if a double-outlet atrium is also present) atrioventricular orifices, or a common atrioventricular orifice, opening into one ventricular chamber, respectively.
High-resolution analyses of early human embryonic development from Carnegie stages 13-23 (representing embryonic days 30-56) [1, 2] have confirmed at least two processes that must go awry to create double-inlet left ventricle (LV): failure of the common (unseptated) atrioventricular canal to move rightward from its "starting" alignment over the eventual LV at day 30 and the contemporaneous failure to form a normal ventricular septum. These two processes may be coupled in human heart development and appear to be independent of atrioventricular canal septation itself because newborns with common-inlet LV are exceedingly rare. Common-inlet right ventricle is uncommon and occurs mostly in the setting of heterotaxy syndrome.
In a remarkable set of experiments, the developmental biologist Benoit Bruneau and his colleagues uncovered the molecular basis for ventricular septum formation. [3] In humans and other mammals, expression of the T-box transcription factor Tbx5 correlates with the formation of the ventricular septum (high in the left ventricle and low in the right, with a sharp boundary of expression exactly at the location where the septum forms). [4] The Tbx5 homozygous null mouse dies at embryonic day 10.5 with a severely hypoplastic LV [5] along with many other defects, reflecting the crucial role this protein has in many aspects of embryonic development.
During early development in the turtle, an animal with only one ventricle, Tbx5 is expressed throughout its lone ventricular chamber. [3] To prove that the level of Tbx5 is causal of ventricular septum formation rather than merely correlative, Bruneau’s laboratory genetically engineered mice to express Tbx5 at a moderate level throughout the developing heart, as in turtles, instead of the normal steep left-right gradient. Offspring from these mice had only a "single ventricle;" although left-right differences in the ventricular expression of downstream genes such as Nppa (atrial natriuretic peptide) persisted, no ventricular septum formed. [3]
By mimicking the turtle pattern of Tbx5, these investigators had created mouse hearts that resembled turtle hearts. Therefore, a sharp line delineating an area of high expression of Tbx5 is critical to induce the formation of a ventricular septum, a precursor for the fashioning of two separate, specialized ventricular compartments. A similar single ventricle phenotype was found by Toshihiko Ogura’s laboratory when they misexpressed Tbx5 in the embryonic chick ventricle. [6]
See the image below.
 A sharp left-right gradient in Tbx5 expression is required for the formation of the ventricular septum. Image from Zina Deretsky, National Science Foundation after Benoit Brueau, the Gladstone Institute of Cardiovascular Disease.
A sharp left-right gradient in Tbx5 expression is required for the formation of the ventricular septum. Image from Zina Deretsky, National Science Foundation after Benoit Brueau, the Gladstone Institute of Cardiovascular Disease.
Until the early 1970s, surgical management did not include separating the pulmonary and systemic circulations. Attempts to septate patients with single ventricle [7] were abandoned by the early 1980s because the surgically placed patch did not grow and ventricular performance remained poor. Modifications of the procedure initially proposed in 1971 by Fontan for tricuspid atresia [8] have been widely adopted over the last four decades. These cavopulmonary or atriopulmonary modifications effectively channel the systemic venous blood directly into the pulmonary arteries. Whether the effect on overall quality of life is superior to that of the more limited palliations used before 1971 is still unclear. [9]
Hepatic and biliary dysfunction with possible cirrhosis, protein-losing enteropathy, and disadvantageous ejection efficiency combined with elevated after load [10] characterize Fontan-type circulation. [11] Other important sequelae include atrial tachyarrhythmias, short stature, thromboembolism, systemic venous-to-pulmonary venous collaterals, systemic artery-to-pulmonary artery collaterals, plastic bronchitis, and esophageal varices. [11] More detailed information about the technical aspects of the modified Fontan operation are available elsewhere. [11, 12]
Pathophysiology
No circulatory derangement is observed in fetal development, because pulmonary circulation and systemic circulation are normally in parallel, with two levels of connection: atrial and ductal. However, lack of separation between pulmonary and systemic circulations causes obvious cyanosis postnatally, with the severity dependent on the degree of coexistent pulmonary outflow tract obstruction. Cases of single ventricle with aortic arch obstruction are the least cyanotic because they never display pulmonary stenosis, although these patients develop poor lower body perfusion as the ductus arteriosus becomes constricted.
Etiology
The cause of single ventricle in humans is unknown.
To date, at least 10 targeted single-gene disruptions in mice have produced a right ventricular (RV) hypoplasia phenotype reminiscent of single left ventricle (LV). These disruptions include global nulls in Nkx2.5; Isl1 [13] ; Mef2c [14] ; dHand (also known as Hand2) [15] ; Fog-2 [16] ; Fgf8 hypomorph [17] ; Foxh1 [18] ; TGF β 2 [19] ; Bop [20] ; and Has2. [21] The Fog -2 null also displays a common atrioventricular orifice situated almost entirely over the future LV (ie, common-inlet ventricle). Whether hypomorphic alleles of the homologous mutations in the human produce a single ventricle phenotype but do not result in embryonic lethality remains to be shown.
Ventricular-specific misexpression of Tbx5 (as discussed in the Background section [3, 6] ) and myocardial-specific inactivation of GATA4 [22] cause single ventricle.
Epidemiology
United States data
Single ventricle occurs in approximately 5 of every 100,000 live births.
Sex- and age-related demographics
No sex disparities are known.
Presentation is generally occurs within the first month of life, although this is dependent on the severity of pulmonary vs systemic outflow tract obstruction.
Prognosis
The majority of patients should survive 20 years. Patients with significant atrioventricular valve regurgitation have a demonstrably poorer outcome.
Treatments for single ventricle (which, as stated earlier in this article, does not include the entity of hypoplastic left heart syndrome) have been refined over the last 30 years, with improved outcomes into early adulthood.
Unlike hypoplastic left heart syndrome, in which the staged approach to reach a cavopulmonary circulation is clearly superior to performing only the first stage (Norwood procedure), the vast majority of patients with single ventricle have a morphologic left ventricle (LV), do not present in extremis, and are relatively stable over many years once initial palliation, including a systemic–to–pulmonary arterial shunt or pulmonary artery banding, is completed and balanced pulmonary/systemic flow ratio is achieved.
A retrospective study (2000-2011) comprising 368 infants with single ventricle who underwent a Norwood procedure and 118 who underwent aortopulmonary shunt operation found similar interstage mortality between the groups. [23] Risk factors for interstage death in infants who underwent the shunt procedure were lower weight at surgery and the presence of arrhythmias compared to the surviving infants.
In another retrospective study (2012-2016) comprising 57 newborns who underwent hybrid stage 1 surgical palliation, interstage remissions were common (75%), with 17% a result of major adverse events. [24] Interstage mortality was 7%.
Whether the cavopulmonary circulation matches or surpasses this quality of life over a 30-year period is still an open question. [25] The long-term effect of a mean systemic venous pressure greater than 10 mm Hg is unknown in the pediatric population.
Morbidity/mortality
The severity and timing of presentation depend not only on the extent of coexistent pulmonary outflow tract stenosis (or, alternatively, aortic obstruction) but also on the reduction in caliber of the ductus arteriosus. [26] The universal utilization of newborn pulse oximetry screening before discharge to home should aid in the identification of those neonates prior to symptom development.
Patients with single ventricles accompanied by genetic and extracardiac anomalies often have additional risk factors (eg, prematurity, low weight) and have a greater risk of prolonged recovery after first-stage palliation, as well as higher hospital and interstage mortality. [27]
Complications
Pleural effusions, pericardial effusions, ascites post Fontan procedure
Long considered the most agonizing early postoperative complication after Fontan completion, thoracic and abdominal effusions often persisted for weeks and frequently impaired cardiac output. Before the early 1990s, these complications threatened to preclude the application of Fontan's principle to the vast majority of patients with single ventricle.
Although the molecular and cellular basis of this complication remains a mystery, surgeons have begun using various less-than-complete Fontan operations as their final stage. [28] The partial hepatic vein exclusion variation used by Lecompte and then by Norwood has largely been abandoned because more than 80% of patients developed intrahepatic venous collaterals that resulted in increasing right-to-left shunts.
Hence, the complete Fontan operation most widely used since the late 1990s is the fenestrated Fontan operation proposed by Laks. Early postoperative effusive complications are greatly reduced following the fenestrated Fontan (lateral tunnel or extracardiac conduit) likely secondary to a lower central venous pressure. However, arterial oxygen saturation is usually in the high 80s or low 90s, rather than the mid 90s seen after nonfenestrated Fontan. Moreover, whether the long-term outcome is superior if the fenestrations are closed in the first few postoperative years (spontaneous, surgical, or by catheter-delivered device) remains an unsettled issue.
Atrial tachyarrhythmias
This is the most prevalent of the numerous late complications following the various modifications of the Fontan operation and may be the heralding sign of hemodynamic deterioration. The basis for this complication is probably multifactorial, [29] and its treatment can be complex because of the frequent coexistence of sinus node dysfunction. Surgical therapy appears to be superior to medical therapy. [30]
Current hypotheses for the etiology of the sinus node dysfunction center on surgical trauma to portions of the sinus node region or its blood supply.
As an alternative to the hemi-Fontan operation, use of the so-called bidirectional Glenn operation, followed subsequently by extracardiac conduit [31] (rather than the lateral tunnel) placement, has failed to reduce the frequency of sinus node dysfunction. This may be because the demarcation of the sinus node region is not macroscopically evident; thus, attempts to avoid it (such as the bidirectional Glenn) may have been unsuccessful.
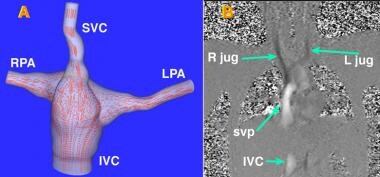 Cardiac magnetic resonance imaging. Frontal view of a three-dimensional flow field in a patient who has undergone a lateral tunnel type of modified Fontan operation (A). This surgical palliation for patients with only one functional ventricle redirects venous blood from the superior vena cava (SVC) and inferior vena cava (IVC) directly into the right (RPA) and left (LPA) pulmonary arteries. Flow streamlines are shown in red. (B.) Frontal view of in plane velocity mapping. Right (R jug) and left (L jug) jugular vein flow towards the feet is signal-poor (black). Flow toward the head in the infrahepatic inferior vena cava (IVC) and intracardiac portion of the systemic venous pathway (svp) is signal-intense (white). Images courtesy of Dr. Mark A Fogel, The Children's Hospital of Philadelphia.
Cardiac magnetic resonance imaging. Frontal view of a three-dimensional flow field in a patient who has undergone a lateral tunnel type of modified Fontan operation (A). This surgical palliation for patients with only one functional ventricle redirects venous blood from the superior vena cava (SVC) and inferior vena cava (IVC) directly into the right (RPA) and left (LPA) pulmonary arteries. Flow streamlines are shown in red. (B.) Frontal view of in plane velocity mapping. Right (R jug) and left (L jug) jugular vein flow towards the feet is signal-poor (black). Flow toward the head in the infrahepatic inferior vena cava (IVC) and intracardiac portion of the systemic venous pathway (svp) is signal-intense (white). Images courtesy of Dr. Mark A Fogel, The Children's Hospital of Philadelphia.
Because the onset of atrial tachyarrhythmia episodes is frequently preceded, if not invariably preceded, by months or years of atrial bradycardia, prophylactic atrial pacing may possibly postpone the emergence of these arrhythmias. Because of the technical challenges of atrial pacing in infants, this proposal has not yet been the subject of a randomized clinical trial.
Hepatic and biliary dysfunction [32, 33]
Liver dysfunction may actually be the underlying etiology for several of the complications listed below (eg, thromboembolism, varices and other venous-to-venous collaterals, thrombocytopenia)
Biliary sludge is the most common finding on gallbladder ultrasonography.
Sinusoidal and portal fibrosis are both seen on biopsy. [34]
Elevated factor VIII, prolonged PT, and elevated GGT are the most sensitive indicators, although other biomarker panels are also currently being evaluated. [35]
Thromboembolism
Venous, but not arterial, thrombosis occurs in nearly 10% of survivors of the fenestrated Fontan operation. The cause of this complication is unknown. Sites can include the pulmonary arteries and the cerebral veins. [36] Subnormal cardiac output, subnormal intracardiac pulsatility of blood flow, and altered hepatic production of components of endogenous thrombolytic pathways have all been proposed as possible etiologies. Hepatic dysfunction, as measured by prothrombin time and galactose elimination half-life, is the rule.
Thrombi have been observed in both the pulmonary venous side of the "lateral tunnel" baffle and the systemic venous side. The presence of a fenestration allows thrombi in the systemic venous circulation to gain access to the systemic arterial circulation.
Aspirin is often prescribed as prophylaxis for venous thrombosis following fenestrated Fontan, and warfarin is gaining acceptance in patients for whom serial measurements of INR are feasible. [37]
Protein-losing enteropathy
Manifesting as diarrhea, poor appetite, or sometimes simply as growth failure, protein-losing enteropathy occurs in at least 10% of long-term survivors of Fontan procedures.
The cause of this usually devastating complication is unknown; however, enteric protein loss starts early after the Fontan operation and is compensated for by increased protein synthesis in the liver so that serum total protein and albumin levels remain in the normal range for a period of time. [38] In fact, by the time the serum albumin falls out of the normal range, severe liver dysfunction has already occurred.
For those with little or no fenestration, fenestration creation (or dilation and stenting) appears to be the most consistently successful palliation, with the improvement sometimes lasting longer than a decade. Atrial pacing has succeeded in at least two cases. Other proposed remedies, including oral steroids and subcutaneous low molecular weight heparin, have succeeded in individual cases but have more numerous adverse effects such as osteopenia. Reduction of both CD4+ and CD8+ T lymphocytes is observed; disproportionate reduction of the CD4+ subset results in a reversal of the CD4+/CD8+ ratio. Immunoglobulin G (IgG) levels and, to a lesser extent, immunoglobulin A (IgA) levels are diminished. [39]
Not observed in the pre-1980 era (when Fontan-type operations were rarely performed), protein-losing enteropathy is thus a result of surgically created cavopulmonary/atriopulmonary circulatory arrangements and is not merely a result of being born with a single ventricle heart.
Persistent discrete or long-segment narrowing of the pulmonary arteries
In the program of staged surgery to reach a fenestrated Fontan, distortions of the pulmonary arteries are not uncommon and should be alleviated either prior to the final stage in the catheterization laboratory or surgically at the time of the final stage.
The importance of identifying cases of Fontan-to-one-lung circulation [40] lies in their vulnerability to the hemodynamic consequences of ipsilateral pulmonary insults. Moreover, 50% of patients with Fontan-to-one-lung circulation develop protein-losing enteropathy, arguing strongly that protein-losing enteropathy is a sequela of Fontan hemodynamics. [41]
Formation of venous collaterals and varices
Patients with single ventricle and the coexistence of interrupted inferior vena cava still have hepatic venous blood that drains to the pulmonary venous side of the circulation after a Kawashima variation of the Fontan procedure.
Collaterals can occasionally form, allowing venous blood from the upper part of the body to eventually reach the pulmonary venous side of the circulation in this subset of patients with single ventricle, as well as in others. Microscopic pulmonary arteriovenous fistulas may also develop in this setting, which is felt to be secondary to absent hepatic blood flow into the pulmonary circulation.
The increased right-to-left shunt can be identified by monitoring either pulse oximetry or hemoglobin levels.
Bronchial wall varices have been observed, possibly due to high superior vena cava pressure. Esophageal varices occur in patients with hepatic dysfunction and portal hypertension.
Low exercise capacity [42]
Although individual exceptions have been observed, the exercise capacity of patients who survive the Fontan procedure, even those with fenestrated variants, is subnormal.
The resting cardiac index is about 70%-80% of normal. Disadvantageous ejection efficiency is present, combined with elevated pulsatile and nonpulsatile components of ventricular afterload. [10]
Short stature
This is observed in patients who survive the Fontan operation even in the absence of documented protein-losing enteropathy. The molecular and cellular basis of this complication is unknown; however, low bone-specific alkaline phosphatase appears to increase when cardiac index is augmented. This suggests that reduced osteoblastic function from subnormal bone perfusion may be the culprit. [43] Whether exogenous growth hormone ameliorates the subnormal growth (but with acceptable incidence of adverse effects) is not known.
Formation of pulmonary arteriovenous malformations
This complication of the hemi-Fontan operation and its variants sometimes resolves after the performance of a less-than-complete Fontan operation (of the lateral tunnel, extracardiac conduit, or hepatic vein exclusion varieties). Contrast echocardiography, which is best performed directly into the pulmonary arteries at the time of cardiac catheterization, appears to be a highly sensitive method of identifying pulmonary arteriovenous malformations. [44]
Plastic bronchitis
This is characterized by the development of mucinous bronchial casts. Palliation by atrial pacing, [45] fenestration creation, [46] or heart transplantation [47] has been reported.
Formation of systemic-to-pulmonary arterial collaterals
Systemic artery-to-pulmonary artery collaterals can carry as much as 40% of the total ventricular output. Whether this is due to the arterial desaturation caused by the prior hemi-Fontan (or bidirectional Glenn) or by the surgically created fenestration is not yet known. [48]
Magnetic resonance imaging is a useful noninvasive diagnostic modality for screening and hemodynamic assessment; however, angiography is usually required for visualization and intervention.
Thrombocytopenia [49]
Whether this is due to deficient thrombopoietin, which is provided by the liver as well as by the kidney, is not yet known. [50]
Patient Education
Because the outcome of various modifications of Fontan operation includes a monotonically increasing prevalence of serious sequelae, discussion with families about prognoses are necessarily lengthy.
Although moderate altitude does not affect early survival after Fontan, [51] living at an altitude of 1700 meters does impair long-term survival. [52]
If the initial identification of single ventricle is made in utero, then the possibility of pregnancy termination may also be introduced to family members.
Finally, the family should confront the possibility that cardiac transplantation may eventually be needed, even if the staged approach to achieve a fenestrated Fontan is the initial strategy adopted.
-
Cranially angulated frontal angiogram of an L-looped single left ventricle (LV). ao = aorta, mpa = main pulmonary artery, oc = outlet chamber (rudimentary right ventricle).
-
Long axial oblique-equivalent subcostal echocardiogram of single left ventricle (vent) with narrow communication (unlabeled arrow) between the left ventricle and outlet chamber (oc). L = left, lav = left atrioventricular valve, P = posterior, rav = right atrioventricular valve, S = superior.
-
Cardiac magnetic resonance imaging. Frontal view of a three-dimensional flow field in a patient who has undergone a lateral tunnel type of modified Fontan operation (A). This surgical palliation for patients with only one functional ventricle redirects venous blood from the superior vena cava (SVC) and inferior vena cava (IVC) directly into the right (RPA) and left (LPA) pulmonary arteries. Flow streamlines are shown in red. (B.) Frontal view of in plane velocity mapping. Right (R jug) and left (L jug) jugular vein flow towards the feet is signal-poor (black). Flow toward the head in the infrahepatic inferior vena cava (IVC) and intracardiac portion of the systemic venous pathway (svp) is signal-intense (white). Images courtesy of Dr. Mark A Fogel, The Children's Hospital of Philadelphia.
-
A sharp left-right gradient in Tbx5 expression is required for the formation of the ventricular septum. Image from Zina Deretsky, National Science Foundation after Benoit Brueau, the Gladstone Institute of Cardiovascular Disease.





