Background
Knowledge of physiology, normal and variant anatomy, and anomalies of coronary circulation is an increasingly vital component in managing congenital and acquired pediatric heart disease. Congenital, inflammatory, metabolic, or degenerative disease may involve coronary circulation, and increasingly complex cardiac surgical repairs demand enhanced understanding to improve operative outcomes.
Variations in coronary anatomy are often recognized in association with structural forms of congenital heart disease. Importantly, coronary artery anomalies are a cause of sudden death in young athletes in the absence of additional heart abnormalities. Understanding the pathophysiology is important in guiding management because variations in coronary anatomy are common. Because of considerable heterogeneity of coronary vasculature, what is considered atypical, abnormal, aberrant, anomalous, accessory, ectopic, incidental, variant, or significant is often unclear. The terms anomalous or abnormal are used to define any variant form observed in less than 1% of the general population.
The Latin term corona, or crown, aptly describes coronary arteries that supply cardiac parenchyma with nutrient blood flow. Coronary arteries (most often two) are normally the only vessels arising immediately above the free margin of aortic valve from the ascending aorta. The name and nature of a coronary artery or branch is defined by that vessel's distal vascularization pattern or territory, rather than by its origin. The right coronary artery (RCA) most commonly arises separately from an ostium just below the sinotubular junction of the right (right anterior) sinus of Valsalva. The normal anatomy of the coronary arteries is shown in the image below.
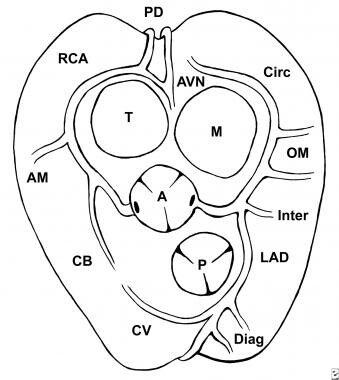 Normal anatomy of coronary arteries, viewed from above with the atria removed. A = aortic valve; P = pulmonary valve; T = tricuspid valve; M = mitral valve; RCA = right coronary artery; AM = acute marginal branch of the right coronary artery; CB = conus branch of the right coronary artery; PD = posterior descending branch; AVN = atrioventricular nodal branch; Circ = circumflex coronary artery; OM = obtuse marginal branches of circumflex coronary artery; LAD = left anterior descending coronary artery; Diag = diagonal branches of the left anterior descending coronary artery; Inter = intermedius branch of the left coronary artery.
Normal anatomy of coronary arteries, viewed from above with the atria removed. A = aortic valve; P = pulmonary valve; T = tricuspid valve; M = mitral valve; RCA = right coronary artery; AM = acute marginal branch of the right coronary artery; CB = conus branch of the right coronary artery; PD = posterior descending branch; AVN = atrioventricular nodal branch; Circ = circumflex coronary artery; OM = obtuse marginal branches of circumflex coronary artery; LAD = left anterior descending coronary artery; Diag = diagonal branches of the left anterior descending coronary artery; Inter = intermedius branch of the left coronary artery.
The RCA courses in the right atrioventricular groove and provides nutrient branches to the right ventricular free wall, extending to the acute margin of the heart. The distal extent of the RCA varies and may extend posteriorly as far as the obtuse margin of the heart. In 90% of patients, the RCA supplies the posterior descending coronary artery branch at the crux of the heart, which supplies the atrioventricular (AV) node and the posterior aspect of the interventricular septum.
The first branch arising from the RCA is the conal or infundibular branch, which courses anteriorly to supply the muscular right ventricular outflow tract or infundibulum. The RCA supplies blood to the atria with a highly variable pattern of small branches. The sinus node artery arises from the proximal RCA in approximately 50% of patients. The left coronary artery (LCA) arises from the mid position of the left (left anterior) sinus of Valsalva (sinuses on either side of the point of aortic and pulmonary commissural contact) just above the level of the free margin of the aortic valve leaflet and generally below the sinotubular junction.
The left coronary ostium is usually single, giving rise to a short, common LCA trunk that branches into the left anterior descending (LAD) and circumflex (Cx) coronary arteries. The LAD courses in the anterior interventricular groove, giving rise to the anterior septal perforating branches as it extends toward the cardiac apex. Small branches may arise from the LAD and supply the anterior wall of the right ventricle. Diagonal branches arise from the LAD and course at downward angles to supply the anterolateral free wall of the left ventricle.
The Cx coronary artery courses along the left AV groove, around the obtuse margin, and posteriorly toward the crux of the heart. Should the Cx coronary reach the crux of the heart and supply the posterior descending coronary artery, the left coronary system would be termed dominant. This occurs in approximately 10% of patients. Atrial branches may arise from the Cx coronary artery and supply the sinus node in 40% of patients. Obtuse marginal branches arise from the Cx system to supply the posterolateral aspect of the left ventricle. In an estimated 70% of patients, a coronary branch (termed ramus medianus, intermedius, or intermediate branch) arises early off the left coronary system to supply an area between diagonal branches from the LAD and obtuse branches from the Cx systems.
Variability in coronary circulation
Despite the position of the heart within the chest and the position of the great arteries as they arise from the heart, aortic and pulmonary valves normally have a single point of contact, with commissural apposition at this point. Coronary arteries almost always arise normally from the "facing" sinuses of Valsalva on either side of this point of commissural contact. Coronary arteries do not normally arise from "nonfacing" or most distant sinus; however, variations in coronary anatomy are common. Variations that occur in less than 1% of the general population may be considered abnormal or anomalies. [1, 2] Coronary artery development, both normal and abnormal, has been reviewed in recent years. [3]
Number and size of coronary ostia
Normally, an individual has two or, sometimes, three coronary ostia. Often, the conal branch of the RCA may arise separately from the right sinus. The Cx or LAD may, on occasion, arise directly from the aortic root. Coronary ostia are typically equal to, or larger than, the vessel they supply.
Positioning within sinuses
Coronary arteries arise more or less perpendicular to the aortic wall. Ostia are located in the middle of the sinus, just above the free leaflet margin of the aortic leaflet and below the sinotubular junction. Coronary arteries that arise ectopically usually course tangentially to the aortic wall or arise in close relationship to the commissure of the aortic valve.
Course of coronary arteries
The course of named coronary arteries is mostly epicardial, although the proximal LAD may have an intramural or subepicardial course in 5-25% of the general population. Branches of epicardial vessels generally proceed in a perpendicular course to supply myocardial arterioles and capillaries. This uniquely designed pattern of epicardial (reservoir) and intramyocardial (nutrient) supply optimizes blood flow to the heart.
Patient education
For patient education resources, see Heart Health Center as well as Tetralogy of Fallot.
Pathophysiology
The heart has a very limited capacity for anaerobic metabolism. The primary source of energy is oxidative metabolism of free fatty acids; therefore, the heart has a negligible ability to tolerate periods of ischemia, yet its capacity to extract oxygen is great (although relatively fixed), and limited degrees of hypoxemia are generally well tolerated. At rest, the oxygen requirement of the heart (8-10 mL/min/100 g) is much greater than of the skeletal muscle (0.115 mL/min/100 g). Exercise requires a 50% increase in oxygen demand primarily met by an increase in myocardial flow 3-4.5 times greater than baseline.
The pattern of coronary blood flow is unique. Epicardial coronary vessels serve as capacitance vessels, primarily filling during the period of diastole (as much as 85% of total flow), and intramural pressure and resistance to myocardial perfusion progressively increase from the outer to inner layers of the heart. Myocardial arterioles have tremendous vasodilatory reserve capacity and enable high flow and low resistance in response to exercise. Recent investigations suggest that the coronary vascular tree has a dual mechanism of vasodilatation: larger proximal vessels by endothelium-derived nitric oxide and direct stimulation of smooth muscle cell alpha2-receptors by adenosine and other metabolites. [4]
A coronary artery with an oblique origin, intramural (within the wall of the aorta) course, or positioning between the great arteries puts the coronary arteries at risk for compression and may significantly limit the reservoir capacity of the epicardial coronary system. Comparable pressure in larger vessels creates greater wall tension and is felt to cause compression of smaller vessels that are in continuity by the Laplace law (tension = pressure X radius).
Proximal areas of significant stenosis hamper the heart's capacity to respond to increased myocardial oxygen demands. The major regulators of coronary blood flow are as follows:
-
Intramural pressure
-
Aortic diastolic perfusion pressure
-
Myocardial metabolic rate (in turn related to heart rate, inotropic state, and systolic arterial pressure)
-
Autonomic nervous system control
-
Endothelial function
-
Blood viscosity in response to decreased myocardial oxygen supply
Myocardial ischemia is the primary manifestation of congenital or acquired coronary artery disease (CAD).
In Coronary Artery Anomalies, Angelini comprehensively classifies coronary anomalies in (normal) human hearts, as follows [5] :
-
Anomalies of origination and course
-
Anomalies of intrinsic coronary arterial anatomy
-
Anomalies of coronary termination
-
Anomalous collateral vessels
Anomalies of origination and course
Anomalies of origination and course include the following [6] :
-
Absent left main trunk (split origination of the left coronary artery [LCA])
-
Anomalous location of coronary ostium within aortic root or near proper aortic sinus of Valsalva (for each artery): High, low, commissural
-
Anomalous location of coronary ostium outside normal "coronary" aortic sinuses
-
Anomalous origination of the coronary ostium from opposite, facing "coronary" sinus (potentially involves joint origination or adjacent double ostia) Variants include the following: (1) the right coronary artery (RCA) arising from the left anterior sinus, with anomalous course; (2) the left anterior descending (LAD) coronary artery arising from right anterior sinus, with anomalous course; (3) the circumflex artery arising from the right anterior sinus, with anomalous course; and (4) the LCA arising from the right anterior sinus, with anomalous course
-
Single coronary artery
For more detailed information, please refer to Angelini P, Velasco JA, Flamm S. Coronary anomalies: incidence, pathophysiology, and clinical relevance. Circulation. 2002 May 21;105(20):2449-54. PMID: 12021235. [6]
Anomalies of intrinsic coronary arterial anatomy
Anomalies of intrinsic coronary arterial anatomy include the following:
-
Congenital ostial stenosis or atresia (LCA, LAD, RCA, Cx): Coronary ostial dimple, coronary ectasia or aneurysm
-
Absent coronary artery
-
Coronary hypoplasia
-
Intramural coronary artery (muscular bridge)
-
Subendocardial coronary course
-
Coronary crossing
-
Anomalous origination of posterior descending artery from anterior descending branch or septal penetrating branch
-
Absent PD (split RCA): Variants include proximal and distal PDs, both arising from the RCA
-
Absent LAD (split LAD): Variants include (1) LAD and a first large septal branch and (2) double LAD
-
Ectopic origination of first septal branch
Anomalies of coronary termination
Anomalies of coronary termination may include inadequate arteriolar/capillary ramifications as well as fistulas from the RCA, LCA, or infundibular artery to the following:
-
Right ventricle
-
Right atrium
-
Coronary sinus
-
Superior vena cava
-
Pulmonary artery
-
Pulmonary vein
-
Left atrium
-
Left ventricle
-
Multiple, right and left ventricles
Epidemiology
United States data
A higher incidence of coronary anomalies is observed in young victims of sudden death than in adults (4-15% vs 1%, respectively). Several large studies address the frequency of minor and major coronary anomalies in different subsets of patients by varying techniques and recording methods. Angelini's comprehensive review identified an incidence of coronary anomalies in 5.6% of consecutive patients undergoing angiographic study and is shown in the image below. [5]
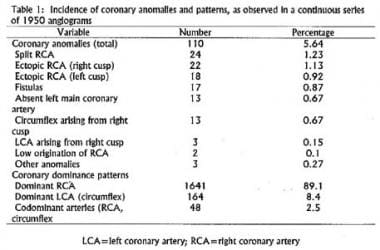 Incidence of coronary artery abnormalities detected in 1,950 selective coronary angiograms performed in adult patients with suspected coronary arterial obstructive disease and otherwise anatomically normal hearts.
Incidence of coronary artery abnormalities detected in 1,950 selective coronary angiograms performed in adult patients with suspected coronary arterial obstructive disease and otherwise anatomically normal hearts.
The most common coronary variants were split RCA (1.23%) and ectopic origin of the RCA near the right aortic sinus (1.13%). Many coronary variations, such as intramural extension or myocardial bridging of the LAD, which occurs in 5-25% of patients, are so common, they are not considered an anomaly.
Anomalous origins of the coronary arteries have been described in siblings, [7] and a recent study suggested a higher incidence of asymptomatic anomalous coronary origins in first-degree relatives of patients with an anomalous coronary, raising the question of whether screening family members should be considered. [8]
In a large retrospective incidence study, coronary artery anomalies were found in 1% of adults and 0.9% of children. [9] Anomalous left circumflex artery was the most common anomaly in adults (25%). The majority of adults were asymptomatic; anomalous left coronary artery from pulmonary artery and myocardial bridges were the only anomalies responsible for anginalike symptoms in adults. In children, anomalous left coronary artery from the pulmonary artery was most common (48%), it was generally detected due to symptoms, and it always required urgent surgical treatment. [9]
Race-, sex-, and age-related demographics
No racial or sexual predisposition is known.
Anomalous origin of the LCA from the pulmonary artery presents in early infancy. Significant coronary anomalies usually result in symptoms or sudden death in older children or young adults. Numerous incidental coronary anomalies may be detected at the time of coronary angiography in later adult life.
Prognosis
Morbidity/mortality
Many coronary anomalies are clinically silent and are recognized only at the time of autopsy. The incidence of incidental coronary anomalies at autopsy includes a single coronary artery in 0.024% and coronary arterial fistulae in 0.2%. After hypertrophic cardiomyopathy, coronary artery abnormalities are the second most common cause of sudden death in young athletes.
-
Incidence of coronary artery abnormalities detected in 1,950 selective coronary angiograms performed in adult patients with suspected coronary arterial obstructive disease and otherwise anatomically normal hearts.
-
Normal anatomy of coronary arteries, viewed from above with the atria removed. A = aortic valve; P = pulmonary valve; T = tricuspid valve; M = mitral valve; RCA = right coronary artery; AM = acute marginal branch of the right coronary artery; CB = conus branch of the right coronary artery; PD = posterior descending branch; AVN = atrioventricular nodal branch; Circ = circumflex coronary artery; OM = obtuse marginal branches of circumflex coronary artery; LAD = left anterior descending coronary artery; Diag = diagonal branches of the left anterior descending coronary artery; Inter = intermedius branch of the left coronary artery.
-
Thirteen patterns of origin and proximal epicardial course of coronary arteries in 255 hearts with complete transposition of the great arteries. LAD = left anterior descending coronary artery; LCA = left coronary artery; LCx = left circumflex coronary artery; RCA = right coronary artery. (Image courtesy of Excerpta Medica, Inc).
-
MRI of anomalous right coronary artery (RCA = black arrow) arising from the left sinus of Valsalva and coursing interatrially between the aorta (AO) and the pulmonary artery (PA). Note the oblique origin and the intramural course within the aortic wall, all factors compromising coronary blood flow.
-
Three-dimensional volume rendering from multidetector CT imaging of a large right coronary artery aneurysm (arrow). Subtraction of the myocardium in B shows the fistula draining to the coronary sinus and then into the right atrium. (Reproduced from Manghat NE, Morgan-Hughes GJ, Marshall AJ, Roobottom CA: Multidetector row computed tomography: imaging congenital coronary artery anomalies in adults. Heart 2005 Dec; 91(12): 1515-22).
-
Selective right coronary arterial injection in an 8-month-old female with tetralogy of Fallot malformation. Study demonstrates left anterior descending coronary artery (LAD) arising early from the right coronary artery (RCA) and coursing across the right ventricular outflow tract. Left anterior oblique projection.
-
Operative repair of anomalous left coronary artery (LCA) from the right sinus of Valsalva. The slitlike anomalous origin of the left coronary artery from the right aortic sinus of Valsalva is demonstrated, as is the intramural course of the coronary artery. (B) The intramural course of the artery is unroofed, placing the functional ostium in the left sinus. (C) Tacking sutures are used to secure the intima of the new coronary ostium and to reinforce the adjacent commissure of the aortic valve. (Reproduced from Jaquiss RD, Tweddell JS, Litwin SB: Surgical therapy for sudden cardiac death in children. Pediatr Clin North Am 2004 Oct; 51(5): 1389-400).





