Background
Aortic valve stenosis results from minor to severe degrees of aortic valve maldevelopment. This stenosis causes mild to severe obstruction of the left ventricular outflow that may be associated with other left heart obstructive lesions, varying degrees of left heart hypoplasia, or extracardiac malformations, including genetic disorders. This article focuses on the presentation, clinical features, and therapeutic options associated with aortic valve stenosis.
An estimated 10%-15% of patients with aortic valve stenosis present with the condition when they are younger than 1 year due to severe stenosis. The remainder of patients may present later in childhood or in adulthood due to progressive obstruction. Adult patients with bicuspid aortic valves may develop significant stenosis or insufficiency after the valve becomes calcified (as seen in the image below), in the fourth, fifth, or sixth decade of life.
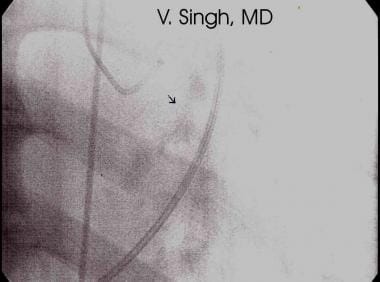 Valvular calcification of aortic stenosis is seen with cardiac fluoroscopy during catheterization.
Valvular calcification of aortic stenosis is seen with cardiac fluoroscopy during catheterization.
Bicuspid aortic valves without stenosis or insufficiency in adult patients can be associated with progressive pathologic enlargement of the aortic root of uncertain etiology. This may require surgical root replacement once the aorta reaches a specific diameter.
In the neonate, transthoracic echocardiography provides complete diagnostic and hemodynamic information. In older patients, transthoracic echocardiography is usually diagnostic; in rare cases, however, a large adolescent patient may require transesophageal echocardiography to clearly delineate the left ventricular outflow tract and to detail the valve anatomy. Cardiac catheterization is usually performed in anticipation of balloon aortic valvuloplasty (see Workup).
Balloon aortic valvuloplasty is considered the initial treatment of choice in pediatric patients with congenital aortic valve stenosis. Surgical repair or replacement of an aortic valve is primarily reserved for patients in whom balloon valvuloplasty has failed with severe stenosis or have significant valve insufficiency in association with progressive left ventricular dilation or deterioration of left ventricular systolic function (see Treatment).
Go to Aortic Stenosis, Pediatric Supravalvar Aortic Stenosis, and Pediatric Subvalvar Aortic Stenosis for more complete information on these topics.
Anatomy
In patients with aortic valve stenosis, most commonly the valve is bicuspid with a single fused commissure and an eccentrically placed orifice. A third or rudimentary commissure may sometimes be apparent.
Less commonly, the valve is unicuspid and dome shaped, particularly in the neonate. Rarely, the valve has three unseparated cusps, with the stenosis being centrally located. Secondary calcification of the valve is extremely rare in childhood, and at times, the aortic valve anulus may also be underdeveloped or hypoplastic in association with mitral and left ventricular hypoplasia, adding to the severity of left ventricular outflow tract (LVOT) obstruction.
Pathophysiology
Pure aortic valve stenosis results in compensatory ventricular hypertrophy over time proportional to the degree of obstruction. Mild-to-moderate degrees of obstruction are usually well tolerated, with minimal hypertrophy and normal left ventricular function. As stenosis progresses, often in association with periods of rapid somatic growth, hypertrophy increases along with wall stress. With severe hypertrophy and valvar obstruction, myocardial ischemia may result from the combination of limited cardiac output, reduced coronary perfusion, and increased myocardial oxygen consumption. A small, fixed, cross-sectional area of the aortic valve can limit the ability to increase cardiac output with exercise. This may result in exercise-induced syncope or sudden death.
Severe obstruction in utero may lead to variable degrees of left-sided heart hypoplasia, endomyocardial fibroelastosis, reduced ventricular function, and significant mitral valve insufficiency.
Yetman et al described neonatal patients in whom rapid progression of aortic stenosis occurred within 6 months of diagnosis. [1] These patients often had well-preserved ventricular function but, during rapid growth, could exhibit fairly dramatic increases in the aortic valve gradient, requiring intervention. The typical absence of symptoms in this age group, does not correlate with the severity of aortic valve obstruction.
Spontaneous development of significant aortic insufficiency in the absence of stenosis is less common and may result in ventricular dilation. This could be associated with a recent episode of bacterial endocarditis. Rarely, left ventricular dysfunction and symptomatic congestive heart failure occur unless stenosis is reduced and/or insufficiency is relieved.
Etiology
Causes of aortic valve stenosis are multifactorial, although studies suggest a higher rate of recurrence of left ventricular outflow tract obstructive lesions in the offspring than other forms of congenital heart disease. The recurrence risk in offspring of an affected father is approximately 3% but is approximately 15% in offspring of an affected mother. Abnormal fetal hemodynamics are theorized to contribute to the development of aortic valve stenosis and other left-sided heart obstructive lesions.
Similarly, other forms of left heart obstructive disease may occur repeatedly within families (eg, hypoplastic left heart syndrome in a child whose older sibling had coarctation of the aorta). A definite genetic defect for aortic valve stenosis has not been identified, but the presence of a bicuspid aortic valve has been documented in multiple family members and is a common congenital heart defect in patients with Turner syndrome (monosomy X).
Epidemiology
The crude incidence of congenital heart defects is approximately 8 per 1000 live births. Aortic valve stenosis accounts for 3%-5% of all congenital heart defects. Authorities estimate a bicuspid aortic valve is present in as many as 1% of the general population, although accurate figures regarding prevalence of this abnormality are difficult to obtain, because many cases remain undetected and these valves function well for many decades.
Some studies have documented a higher prevalence of aortic valve stenosis in white children than in black and Hispanic children. There is a strong male sex predilection in aortic valve stenosis: the male-to-female ratio is 4:1.
Prognosis
The prognosis for patients with congenital aortic valve stenosis depends on the valve anatomy and its response to intervention. The severity of the disorder is widely varied, ranging from no symptoms in patients with a bicuspid aortic valve and no stenosis to critical illness in neonates.
Mortality is higher in patients presenting with severe or critical aortic valve stenosis during the first year of life, specifically in the neonatal period, although this risk has decreased significantly over the past 20 years. Mortality is in part influenced by associated congenital cardiac anomalies, which occur in as many as 20% of patients. These include coarctation of aorta, ventricular septal defect, mitral valve stenosis or insufficiency, and left ventricular hypoplasia. Undetected, severe aortic valve stenosis is a known cause of sudden death and accounts for approximately 1% of all causes of sudden death in young people.
A retrospective cohort study in 245 patients with congenital valvular aortic stenosis by Ten Harkel et al found that mortality was high for patients who were diagnosed in infancy but was almost absent in those who were diagnosed after infancy. [2] Interventions were required more often in children diagnosed at a younger age and/or with higher gradients.
Patient Education
Education is indicated for affected families regarding signs of progressive aortic stenosis, heart failure, and low cardiac output. Education regarding good dental care and avoidance of risk factors for endocarditis is imperative.
Other goals of parent education include setting reasonable goals for exercise participation that allow for a healthy lifestyle but downplay long-term goals for competitive athletics or strenuous isometrics at a high level until significant relief of aortic valve disease is accomplished by aortic valve repair (balloon valvuloplasty versus surgical) or replacement.
Competitive aerobic sports are prohibited in patients with severe aortic valve stenosis, whereas patients with mild stenosis can participate if they have normal electrocardiogram findings, exercise tolerance, and no history of exercise induced chest pain, syncope, or tachyarrhythmias. Patients with moderate aortic valve stenosis may also participate in low-to-moderate dynamic competitive sports, if certain conditions are met. [3]
Similarly, emphasize that treatment for aortic valve disease is a lifelong process and is best introduced early and reinforced often to ensure that patients with aortic valve stenosis continue to receive ongoing follow-up care as they make the transition from an adolescent lifestyle at home to the independence of young adulthood.
-
Valvular calcification of aortic stenosis is seen with cardiac fluoroscopy during catheterization.





