Background
Aortic valve insufficiency results from leakage and backflow of blood that is ejected from the left ventricle (LV) into the ascending aorta back into the left ventricle.
Many mechanisms contribute to aortic valve insufficiency. These include abnormalities of the aortic valve leaflets and pathologies of the proximal aortic root. This article primarily focuses on aortic valve insufficiency caused by abnormalities in the aortic valve leaflets.
Anatomy of the aortic valve
The aortic valve is composed of 3 thin leaflets (ie, cusps) that project from the wall of the proximal ascending aorta. These leaflets and their respective sinuses of Valsalva are termed left, right, and noncoronary.
Embryologic development of the aorta
In the embryonic stage, the truncus arteriosus connects to the dorsal aspect of the aorta via 6 pairs of aortic arches. The separation of truncus arteriosus into 2 great arteries results from the fusion of the aorticopulmonary septum and the truncus septum. The semilunar valves and their related sinuses are created by absorption and the hollowing out of tissue at the distal side of the truncus ridges.
Many mouse single-gene-knockout models of truncus arteriosus have been reported (eg, Sox4 null, Tbx1 null, pax3Splotch), although only NFATc1 null and Sox4 null display absent semilunar cusps. Ablation of a particular region in the cranial neural crest also results in truncus arteriosus, at least in the chick.
Aortic valve insufficiency can be due to, or associated with, congenital heart disease.
-
Ventricular septal defect of the membranous (conoventricular) or conal septal (infundibuloventricular) types
-
Bicuspid (ie, bicommissural) aortic valve [1]
-
Subvalvular aortic stenosis
-
Dysplasia of valve cusps, without fusion of commissures
-
Absence of 2 or 3 aortic valve leaflets
Acquired valvular aortic insufficiency
Causes of acquired aortic valve insufficiency include endocarditis, trauma, systemic diseases, and connective tissue syndromes. Systemic diseases that cause aortic valve insufficiency include the following:
Syndromes that lead to aortic valve insufficiency include the following:
-
Ehlers-Danlos syndrome, type IV
Recently, the percentage of individuals with aortic valve insufficiency caused by aortic root disease has been steadily increasing compared with the percentage of those with valvular disease. In fact, more than half of patients who present with pure aortic regurgitation (AR) without any associated cardiac anomalies have aortic valve insufficiency caused by aortic root disease. See the image below.
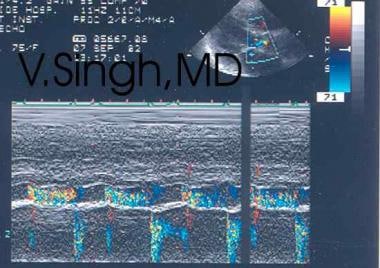 Aortic regurgitation. Color Doppler echocardiogram.
Aortic regurgitation. Color Doppler echocardiogram.
Pathophysiology
Regardless of etiology, aortic valve insufficiency results in volume overload on the LV because the LV is forced to pump the entire diastolic volume received from the left atrium and the regurgitant volume from the aorta through an incompetent aortic valve. Over time, such volume overload (ie, increased preload) causes eccentric hypertrophy of the LV. (Compare this with the concentric hypertrophy observed in aortic stenosis.)
Chronic aortic insufficiency
In long-standing aortic regurgitation, this compensatory mechanism begins to deteriorate. When LV function cannot continue to compensate for volume overload, the LV dilates, and LV end-diastolic volume increases, even without further increase in aortic regurgitation volume. The LV thickness–to–chamber size ratio decreases. This causes an increase in systolic wall tension and a decrease in ejection fraction, stroke volume, and ventricular emptying. This larger end-systolic volume leads to progressively larger end-diastolic volume.
With progressive increases in wall tension, a mismatch occurs between oxygen demand and supply. Supply, which is always abnormally tenuous because of the lower-than-normal coronary driving pressure (difference in aortic diastolic pressure and ventricular diastolic pressure), cannot keep up with the increased demand. Interstitial fibrosis begins to occur, reducing wall compliance and further increasing end-diastolic LV pressure. If untreated, this interstitial fibrosis leads to elevated left atrial pressure and pulmonary venous congestion, especially during exercise. Ventricular ectopy is another manifestation of the oxygen supply-demand mismatch.
Acute severe aortic insufficiency
In acute severe aortic valve insufficiency due to endocarditis or sudden trauma, the LV cannot immediately respond with increased stroke volume to facilitate proper emptying because the element of eccentric hypertrophy is missing. As a result, LV diastolic pressure suddenly rises. Volume overload in the LV results in an early closure of the mitral valve during diastole. This occurs as a natural defense mechanism to protect the pulmonary venous system from the high-pressure regurgitant backflow coming from the high-pressure LV chamber.
Systolic pressures remain effectively unchanged in the aorta and the LV. Because of the increase in LV diastolic pressure, the pulse pressure may not significantly widen in acute severe aortic valve insufficiency. Tachycardia and early closure of the mitral valve are the compensatory mechanisms here.
Natural history
The natural history of aortic valve insufficiency after diagnosis is as follows:
-
Asymptomatic patients with normal LV systolic function
The 5-year survival rate is approximately 75%.
The 10-year survival rate is approximately 50%.
Progression to symptoms, LV dysfunction, or both occurs in fewer than 6% of patients per year.
Progression to asymptomatic LV dysfunction occurs in fewer than 3.5% of patients per year.
Sudden death occurs in fewer than 0.2% of patients per year.
-
Asymptomatic patients with LV systolic dysfunction: Progression to cardiac symptoms occurs in more than 25% of patients per year.
-
Symptomatic patients: The mortality rate is higher than 10% per year.
Most findings in patients with aortic valve insufficiency are related to LV volume overload and eventual myocardial dysfunction.
Individuals with chronic aortic valve insufficiency may be asymptomatic for several years. This is because of adaptation of the LV to the pressure dynamics generated from long-standing volume overload. Many patients with chronic aortic valve insufficiency are no longer in the pediatric age group by the time signs and symptoms appear.
However, in acute severe aortic valve insufficiency, the LV does not have the ability to adapt to sudden volume overload resulting from aortic valve insufficiency. In this setting, LV failure and cardiac collapse occur. They are manifested as chest discomfort, dyspnea, and hypotension.
Epidemiology
Frequency
United States
An estimated 5 million Americans have at least one form of heart valve disease. In 2000, 1 million Americans were affected by congenital heart disease. This is a 3-fold increase from 300,000 in 1980. This figure is projected to increase to 1.4 million in the year 2020. Risk of premature death, complications, and the need for medication because of congenital heart disease is at least 50%.
In approximately two thirds of patients with aortic regurgitation, the disease is rheumatic in origin, resulting in thickening, deformation, and shortening of the individual aortic valve cusps. This leads to changes that prevent their proper opening during systole and closure during diastole. A rheumatic origin is less common in patients with isolated aortic regurgitation.
International
Data are similar to those of the United States. Acute rheumatic fever is associated with varying degrees of valvulitis and myocarditis. A New Zealand study focused on LV mechanics during and after acute rheumatic fever. [2] The study found that the contractile dysfunction during and after acute rheumatic fever evolves in a manner dependent on the degree and type of aortic valve insufficiency and may be influenced by surgical intervention. The study concluded that mechanical factors are the most important contributors to myocardial damage during and after an episode of acute rheumatic fever in children.
Mortality/Morbidity
Mortality and morbidity associated with aortic valve insufficiency are related to the following parameters:
-
Duration of aortic valve insufficiency
-
Severity of valve incompetence
-
Compensatory mechanisms
-
Postsurgical complications for valve replacement in symptomatic severe aortic valve insufficiency
In patients with chronic aortic valve insufficiency, in whom LV diastolic function remains stable and compensatory mechanisms have evolved over time, the presence of a new acute lesion may adversely affect the LV dysfunction. This can have a significant impact on valve function and blood flow dynamics and may ultimately facilitate decompensation. Therefore, even a person with compensated chronic severe aortic valve insufficiency should be considered at a high risk of decompensation with respect to life-threatening cardiac complications. Furthermore, because of the lower-than-normal coronary driving pressure, patients with severe aortic valve insufficiency are difficult to successfully resuscitate following cardiovascular collapse.
Most natural history data are from the adult population with a history of several years of aortic valve insufficiency. According to these data, in patients who have angina, the 5-year survival rate of uncorrected severe aortic valve insufficiency is 50%. Once syncope develops, almost 50% of patients who do not undergo correction die within 3 years. Once heart failure develops, 50% of uncorrected patients die within 2 years. Compare this with an approximate 1-5% mortality rate in patients with surgical correction.
Race
No racial predilection is reported.
Sex
Approximately three fourths of patients with pure or predominant aortic valve insufficiency are males. In patients who have associated mitral valve disease, the incidence is higher in females than in males.
Age
Other than aortic valve insufficiency associated with congenital heart disease, the incidence of aortic valve insufficiency is not age related.
-
Aortic regurgitation. Color Doppler echocardiogram.





