Practice Essentials
Trichuris trichiura, also known as whipworm, acquired the name for the distinctive resemblance of the adult worm to the handle and lash of a whip.
 Adult T trichiura worm removed during a colonoscopy. Courtesy of the CDC (http://phil.cdc.gov/phil/home.asp).
Adult T trichiura worm removed during a colonoscopy. Courtesy of the CDC (http://phil.cdc.gov/phil/home.asp).
It is a roundworm of the phylum Nematoda. [1] Along with hookworm and Ascaris, whipworm constitutes soil-transmitted helminths (STH) and contributes to the major disease burden worldwide. [2]
The organism is spread via the fecal-oral route. Potential hosts ingest the embryonated (mature) eggs. Most heavy infections are observed in the pediatric population because children are more likely to have poor hygiene and to play in soil that carries the worms' mature eggs.
Signs and symptoms
Gastrointestinal symptoms associated with T trichiura infection range from mild to severe. Most infections are asymptomatic.
See Presentation for more detail.
Diagnosis
Diagnosis is based on the microscopic detection of eggs or larvae in fresh or fixed stool samples.
See Workup for more detail.
Management
Treatment with broad-spectrum anthelminthic agents is key. Most infections can be treated successfully with mebendazole, albendazole, or ivermectin.
See Treatment and Medication for more detail.
Pathophysiology
Humans are the only known host of T trichiura and no animal reservoir is recognized.
The organism is spread via the fecal-oral route via ingestion of embyronated eggs with contaminated food or contact with contaminated hands. After ingestion the eggs hatch in the small intestine into the larval form, which penetrate the small intestinal mucosa.
After approximately one week, the immature worms move passively to the large intestine and proximal colon and penetrate the mucosal epithelial cells. The worm continues to expand intracellularly creating tunnels in the epithelium. The posterior end of the worm eventually ruptures the cell membrane and the worm protrudes partially into the lumen of the large intestine, while the anterior part still imbedded in the epithelium. Thus, the worm disrupts the normal colonic architecture; however, the host inflammatory response is the major contributor to the pathogenesis of the worm infection.
About 3 months after the ingestion, the fertilized female worm starts laying eggs. The female worm is capable of producing 3,000-20,000 eggs a day. The infected host passes unembryonated eggs in their feces and the maturation of eggs requires warm humid environment. Egg maturation occurs in approximately 2-6 weeks. T trichura eggs are bile-stained and have a characteristic barrel-shape with the presence of polar plugs in the egg shell. The embryonated egg can maintain viability for several months under suitable conditions. Destruction occurs with exposure to direct sunlight for more than 12 hours and to temperatures of less than -8°C or higher than 40°C for one hour.
The adult worm usually reaches 3-5 cm in length and has a lifespan of 1-3 years.
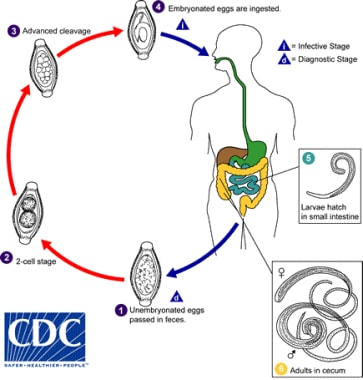 Life cycle of whipworm. The unembryonated eggs are passed with the stool (1). In the soil, the eggs develop into a 2-cell stage (2), an advanced cleavage stage (3), and then they embryonate (4). Eggs become infective in 15 to 30 days. After ingestion in soil-contaminated hands or food, the eggs hatch in the small intestine, and release larvae (5) that mature and establish themselves as adults in the colon (6). The adult worms (approximately 4 cm in length) live in the cecum and ascending colon. The adult worms are fixed in that location, with the anterior portions threaded into the mucosa. The females begin to oviposit 60 to 70 days after infection. Female worms in the cecum shed between 3,000 and 20,000 eggs per day. The life span of the adults is about 1 year. Courtesy of the CDC (http://phil.cdc.gov/phil/home.asp).
Life cycle of whipworm. The unembryonated eggs are passed with the stool (1). In the soil, the eggs develop into a 2-cell stage (2), an advanced cleavage stage (3), and then they embryonate (4). Eggs become infective in 15 to 30 days. After ingestion in soil-contaminated hands or food, the eggs hatch in the small intestine, and release larvae (5) that mature and establish themselves as adults in the colon (6). The adult worms (approximately 4 cm in length) live in the cecum and ascending colon. The adult worms are fixed in that location, with the anterior portions threaded into the mucosa. The females begin to oviposit 60 to 70 days after infection. Female worms in the cecum shed between 3,000 and 20,000 eggs per day. The life span of the adults is about 1 year. Courtesy of the CDC (http://phil.cdc.gov/phil/home.asp).
Epidemiology
United States statistics
Prevalence of whipworm infestation is less than 0.1%, although adequate studies are quite outdated. [3] The most common areas of infection are the southern Appalachian range and Gulf coast states. [4]
International statistics
CDC estimated 604-795 million people in the world are infected with whipworm.
The highest prevalence rates of soil-transmitted helminthes occur in sub-Saharan Africa and southern and eastern Asia. [2] As with other soil-transmitted helminthes, the prevalence is higher in tropical and subtropical regions of the world, which provide the moist, humid environment required for the eggs to mature. Due to the poor sanitation practices in the rural areas of these regions the disease is prevalent.
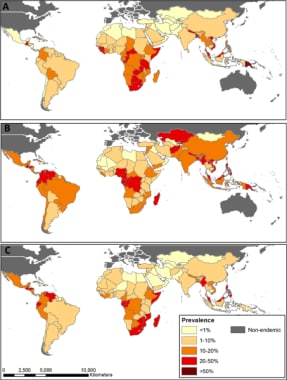 Distribution of soil transmitted helminths (STH) Trichuris trichiura infection prevalence in 2010 based on geostatistical models for sub-Saharan Africa and available empirical information for all other regions. Courtesy of Parasites & Vectors (Pullan RL, Smith JL, Jasrasaria R, Brooker SJ. Global numbers of infection and disease burden of soil transmitted helminth infections in 2010. Parasit Vectors. 2014;7:37).
Distribution of soil transmitted helminths (STH) Trichuris trichiura infection prevalence in 2010 based on geostatistical models for sub-Saharan Africa and available empirical information for all other regions. Courtesy of Parasites & Vectors (Pullan RL, Smith JL, Jasrasaria R, Brooker SJ. Global numbers of infection and disease burden of soil transmitted helminth infections in 2010. Parasit Vectors. 2014;7:37).
Age-related demographics
Although infections are observed in all age groups, most heavy infections are observed in the pediatric population. This probably reflects the increased likelihood of children to have poor hygiene and to play in soil that carries the worms' mature eggs.
Prognosis
With treatment, prognosis is typically excellent.
Morbidity/mortality
Most infections are asymptomatic. Symptoms are related to the worm load or number of worms involved in an infection. Heavy infections (hundreds to thousands of worms) can lead to death secondary to GI and hematologic complications.
Mortality can result from complications such as intestinal obstruction or rectal prolapse requiring surgical intervention.
Morbidity is directly related to worm burden. Soil-transmitted helminths impair the nutritional status of the host due to intestinal bleeding, diarrhea or dysentery and malabsorption of nutrients resulting in growth delay and failure to thrive.
An estimated $4.98 million per year is lost due to disability (YLD) attributable to soil-transmitted helminths worldwide. About 13% is attributable to T trichiura. [5]
Complications
Rectal prolapse, dysentery, anemia, malnutrition, and growth retardation all can complicate heavy infections. In developing countries, T trichiura infection is a common cause of stunting and wasting among children aged younger than 5 years. [6]
Patient Education
Emphasize good hygiene and avoidance of pica. Proper disposal of fecal material needs to be emphasized.
-
Adult T trichiura worm removed during a colonoscopy. Courtesy of the CDC (http://phil.cdc.gov/phil/home.asp).
-
Life cycle of whipworm. The unembryonated eggs are passed with the stool (1). In the soil, the eggs develop into a 2-cell stage (2), an advanced cleavage stage (3), and then they embryonate (4). Eggs become infective in 15 to 30 days. After ingestion in soil-contaminated hands or food, the eggs hatch in the small intestine, and release larvae (5) that mature and establish themselves as adults in the colon (6). The adult worms (approximately 4 cm in length) live in the cecum and ascending colon. The adult worms are fixed in that location, with the anterior portions threaded into the mucosa. The females begin to oviposit 60 to 70 days after infection. Female worms in the cecum shed between 3,000 and 20,000 eggs per day. The life span of the adults is about 1 year. Courtesy of the CDC (http://phil.cdc.gov/phil/home.asp).
-
Distribution of soil transmitted helminths (STH) Trichuris trichiura infection prevalence in 2010 based on geostatistical models for sub-Saharan Africa and available empirical information for all other regions. Courtesy of Parasites & Vectors (Pullan RL, Smith JL, Jasrasaria R, Brooker SJ. Global numbers of infection and disease burden of soil transmitted helminth infections in 2010. Parasit Vectors. 2014;7:37).
-
Rectal prolapse in a female child due to a parasitic Trichuris trichiura infestation. Courtesy of the CDC (http://phil.cdc.gov/phil/home.asp).
-
Egg from the "human whipworm". Courtesy of the CDC (http://phil.cdc.gov/phil/home.asp).





