Practice Essentials
Thromboembolism, or the development of a clot within blood vessels, can occur in arteries or veins. Venous thromboembolism, a leading cause of adult morbidity and mortality, has a lower incidence in children than in adults and carries significant morbidity in both. Arterial thromboembolism is less common in children and will be briefly addressed in this article. (See Epidemiology and Prognosis.)
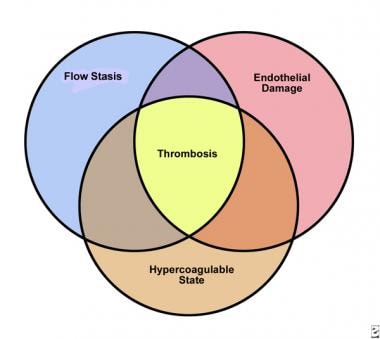
In 1845, Virchow postulated that three factors were important in the development of thrombosis: (1) impairment of blood flow (stasis), (2) vascular injury, and (3) alterations of the blood (hypercoagulability). The Virchow triad still holds true to some extent in addressing the etiology of thrombosis in adults and children (see the diagram below). (See Etiology.)
A high index of suspicion for thromboembolism is required for timely diagnosis; indeed, many early reports on this condition were based on autopsy data. Symptoms of pulmonary embolism (PE) can be nonspecific and may include tachypnea, tachycardia, fever, pleuritic chest pain, cough, shortness of breath, and (less commonly) hemoptysis. Deep venous thrombosis (DVT) is absent in children with PE more often than it is in adults. (See Presentation and Workup.)
Risk factors for thromboembolism include the presence of a central venous catheter, immobility, heart disease, a ventriculoatrial shunt, trauma (especially fractures), cancer, surgery, infection, dehydration, shock, estrogen-containing contraceptives, pregnancy, smoking, and obesity. (See Etiology.) [1]
The diagnosis and treatment of thrombosis in children were initially based on standards of care for adults. However, since the early 1990s, pediatric data have emerged that stress differences in thromboembolism etiology, pathophysiology, and anticoagulant drug pharmacokinetics in children. (See Etiology, Presentation, Workup, Treatment, and Medication.)
Physiology
The physiology of hemostasis is remarkably complex and reflects a fine balance between an uninterrupted flow of blood (ie, fluid) and a rapid, localized response to vascular injury (ie, clotting).
The process of hemostasis is traditionally divided into a cellular phase (primary hemostatic phase) and a fluid phase (secondary hemostatic phase). The former involves platelets and the vascular wall, and the latter involves plasma proteins.
The fluid phase is divided into the following 3 processes, abnormalities in any of which can contribute to hypercoagulable or hypocoagulable states (see the diagram below):
-
The multiple-step zymogen pathway that leads to thrombin generation
-
Thrombin-induced formation of a fibrin clot
-
Complex fibrinolytic mechanisms aimed at limiting clot propagation
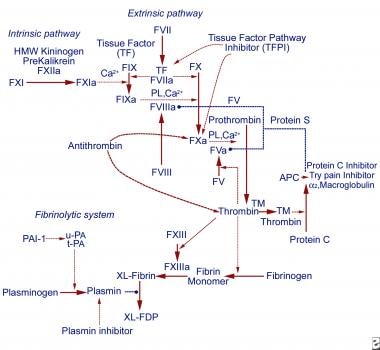 Coagulation cascade. Solid arrows represent activation events, dashed arrows represent inhibition events, and dotted lines with circles represent inactivation events. a = active; APC = activated protein C; F = factor; FDP= fibrin degradation products; HMW = high molecular weight; PAI-1 = plasminogen activator inhibitor-1; PL = phospholipid; TM = thrombomodulin; t-PA = tissue type plasminogen activator; u-PA = urokinase plasminogen activator; XL= crosslinked.
Coagulation cascade. Solid arrows represent activation events, dashed arrows represent inhibition events, and dotted lines with circles represent inactivation events. a = active; APC = activated protein C; F = factor; FDP= fibrin degradation products; HMW = high molecular weight; PAI-1 = plasminogen activator inhibitor-1; PL = phospholipid; TM = thrombomodulin; t-PA = tissue type plasminogen activator; u-PA = urokinase plasminogen activator; XL= crosslinked.

Regarding the fluid phase, many age-dependent differences are present in the hemostatic system of infants and children. Adult levels of the vitamin-K–dependent coagulation factors II, IX, and X, as well as contact factors, are not achieved until age 3-6 months. levels of thrombin inhibitors, such as antithrombin and heparin cofactor II, are similarly low at birth; that is, they are in the ranges that increase the risk for heterozygous adults to develop thromboembolism.
levels of alpha-2-macroglobulin are higher in infants and children than in adults. Conversely, levels of protein C and S are low at birth. Protein S levels approach adult values by age 3-6 months, but protein C levels remain low even into childhood. Plasminogen levels are low in newborns and infants, which has implications for treatment of thromboembolism in newborns. Thrombin generation is decreased (probably because of low prothrombin levels) and delayed in newborns, who have a higher risk for bleeding relative to adults.
Signs and symptoms of pediatric thromboembolism
Although deep venous thrombosis (DVT) is frequently asymptomatic, signs of the condition can include the following:
-
Leg or arm edema
-
Erythema
-
Increased warmth
-
Palpable cord
-
Tenderness
-
Positive Homans sign (ie, pain on dorsiflexing the foot)
Signs of pulmonary embolism (PE) are nonspecific and include the following:
-
Apprehension
-
Diaphoresis
-
Tachycardia
-
Tachypnea
-
Chest pain
-
Hypotension
Signs of arterial thrombosis include absent or diminished peripheral pulses and a cool extremity with or without mottling of the skin.
Workup in pediatric thromboembolism
Laboratory studies
Once a clot is documented, the patient's workup should include the following:
-
Complete blood count (CBC) with peripheral blood smears
-
Measurement of the prothrombin time (PT), activated partial thromboplastin time (aPTT), and fibrinogen level
-
D-dimer measurement
First-line workup for hypercoagulation should include evaluations of the following:
-
Activated protein C resistance and/or the factor V Leiden mutation
-
Protein C
-
Free and total protein S
-
Antithrombin
-
Lupus anticoagulant (which may be screened by using the dilute Russell viper venom test)
-
Anticardiolipin antibodies
-
Prothrombin gene 20210A mutation
-
Lipoprotein(a) levels
-
Plasma homocysteine values (which can be measured after fasting or at 4 h after a loading dose of methionine 100 mg/kg)
Imaging studies
These include the following:
-
Contrast venography - Considered the reference standard for documenting DVT in children
-
Duplex ultrasonography or real-time B-mode ultrasonography with color Doppler imaging - Duplex ultrasonography is increasingly being used as the primary diagnostic tool to confirm thrombosis in adults and children
-
Ventilation-perfusion (V/Q) scanning - Used to be the procedure of choice in children with suspected PE; has largely been replaced by computed tomography (CT) scanning and magnetic resonance angiography (MRA)
-
Magnetic resonance imaging (MRI) and MRA of the head - The modalities of choice for evaluating a child with suspected central nervous system (CNS) thrombosis
-
Head CT scanning with intravenous contrast enhancement - Sometimes useful for detecting sinovenous thrombosis
-
Chest radiography - More helpful for suggesting alternative diagnoses, such as pneumonia, than for diagnosing thromboembolism
Management of pediatric thromboembolism
Anticoagulation is begun with unfractionated heparin (UFH) or low–molecular-weight heparin (LMWH), followed by oral anticoagulation with warfarin.
In June 2021, the US Food and Drug Administration (FDA) approved the oral thrombin inhibitor dabigatran (previously approved for adults) for the treatment of venous thromboembolic events (VTEs) in pediatric patients aged 3 months to under 18 years who have undergone at least 5 days of treatment with a parenteral anticoagulant. Another indication is reduction in the risk of recurrent VTEs in this population.
A patient's medication may include heparin or LMWH, [2] oral anticoagulants, thrombolytic agents, and, occasionally, antiplatelet agents (for arterial thrombosis). Avoid giving antiplatelet agents to children receiving anticoagulation unless they are absolutely necessary.
On occasion, surgical thrombectomy may be required, especially after major cardiac surgery or if thrombolytic agents fail or are contraindicated, or if a limb or organ are threatened.
Patient education
Clearly define activity restrictions, especially in the case of adolescents. If a child is receiving oral anticoagulation, review the vitamin K content of various foods with the family. The proper fitting and need for daily use of compression stockings to prevent post-thrombotic syndrome after lower extremity venous thrombosis must be emphasized. After venous thrombosis occurs, the recurrence risk can be minimized by avoiding additional risk factors, so patients should receive education focused on reducing obesity, avoiding smoking, avoiding oral contraceptives, and, during pregnancy, close monitoring or (if needed) prophylactic therapy.
Background
Thromboembolism, or the development of a clot within blood vessels, can occur in arteries or veins. Venous thromboembolism, a leading cause of adult morbidity and mortality, has a lower incidence in children than in adults and carries significant morbidity in both. Arterial thromboembolism is less common in children and will be briefly addressed in this article. (See Epidemiology and Prognosis.)
In 1845, Virchow postulated that three factors were important in the development of thrombosis: (1) impairment of blood flow (stasis), (2) vascular injury, and (3) alterations of the blood (hypercoagulability). The Virchow triad still holds true to some extent in addressing the etiology of thrombosis in adults and children (see the diagram below). (See Etiology.)
A high index of suspicion for thromboembolism is required for timely diagnosis; indeed, many early reports on this condition were based on autopsy data. Symptoms of pulmonary embolism (PE) can be nonspecific and may include tachypnea, tachycardia, fever, pleuritic chest pain, cough, shortness of breath, and (less commonly) hemoptysis. Deep venous thrombosis (DVT) is absent in children with PE more often than it is in adults. (See Presentation and Workup.)
Risk factors for thromboembolism include the presence of a central venous catheter, immobility, heart disease, a ventriculoatrial shunt, trauma (especially fractures), cancer, surgery, infection, dehydration, shock, estrogen-containing contraceptives, pregnancy, smoking, and obesity. (See Etiology.) [1]
The diagnosis and treatment of thrombosis in children were initially based on standards of care for adults. However, since the early 1990s, pediatric data have emerged that stress differences in thromboembolism etiology, pathophysiology, and anticoagulant drug pharmacokinetics in children. (See Etiology, Presentation, Workup, Treatment, and Medication.)
Physiology
The physiology of hemostasis is remarkably complex and reflects a fine balance between an uninterrupted flow of blood (ie, fluid) and a rapid, localized response to vascular injury (ie, clotting).
The process of hemostasis is traditionally divided into a cellular phase (primary hemostatic phase) and a fluid phase (secondary hemostatic phase). The former involves platelets and the vascular wall, and the latter involves plasma proteins.
The fluid phase is divided into the following 3 processes, abnormalities in any of which can contribute to hypercoagulable or hypocoagulable states (see the diagram below):
-
The multiple-step zymogen pathway that leads to thrombin generation
-
Thrombin-induced formation of a fibrin clot
-
Complex fibrinolytic mechanisms aimed at limiting clot propagation
Coagulation cascade. Solid arrows represent activation events, dashed arrows represent inhibition events, and dotted lines with circles represent inactivation events. a = active; APC = activated protein C; F = factor; FDP= fibrin degradation products; HMW = high molecular weight; PAI-1 = plasminogen activator inhibitor-1; PL = phospholipid; TM = thrombomodulin; t-PA = tissue type plasminogen activator; u-PA = urokinase plasminogen activator; XL= crosslinked.
Regarding the fluid phase, many age-dependent differences are present in the hemostatic system of infants and children. Adult levels of the vitamin-K–dependent coagulation factors II, IX, and X, as well as contact factors, are not achieved until age 3-6 months. levels of thrombin inhibitors, such as antithrombin and heparin cofactor II, are similarly low at birth; that is, they are in the ranges that increase the risk for heterozygous adults to develop thromboembolism.
levels of alpha-2-macroglobulin are higher in infants and children than in adults. Conversely, levels of protein C and S are low at birth. Protein S levels approach adult values by age 3-6 months, but protein C levels remain low even into childhood. Plasminogen levels are low in newborns and infants, which has implications for treatment of thromboembolism in newborns. Thrombin generation is decreased (probably because of low prothrombin levels) and delayed in newborns, who have a higher risk for bleeding relative to adults.
Patient education
Clearly define activity restrictions, especially in the case of adolescents. If a child is receiving oral anticoagulation, review the vitamin K content of various foods with the family. The proper fitting and need for daily use of compression stockings to prevent post-thrombotic syndrome after lower extremity venous thrombosis must be emphasized. After venous thrombosis occurs, the recurrence risk can be minimized by avoiding additional risk factors, so patients should receive education focused on reducing obesity, avoiding smoking, avoiding oral contraceptives, and, during pregnancy, close monitoring or (if needed) prophylactic therapy.
Etiology
Advances in technology have improved the survival of infants who are born prematurely and of children in intensive care units (ICUs). Approximately 95% of children with DVT and/or PE have one or more underlying risk factors; most have more than one. (A study by Ishola et al reported that 81% of adolescents with thromboembolism had two or more risk factors/comorbidities. [3] ) Therefore, a thorough evaluation is warranted, even when the cause of thromboembolism seems obvious.
A study by Yen et al indicated that in pediatric trauma patients, independent risk factors for venous thromboembolism include older age, blood transfusion, surgery, a higher Injury Severity Score, and a lower Glasgow Coma Scale score. [4]
Use of arterial catheters
The use of arterial catheters is the most common risk factor for arterial thromboembolism in children. Cardiac catheterization through the femoral artery to manage congenital heart disease is a frequent cause.
Prophylaxis with heparin (100-150 U/kg) during the procedure lowers the incidence of thrombosis from 40% to 8% in children younger than 10 years. In neonates, catheterization of the umbilical artery poses risks similar to these. The absolute incidence of thrombosis is 10-90% when angiographic diagnostic methods are used.
Use of central venous catheters
Central venous catheter–associated thrombosis was reported in 29% of children in a report by Nuss et al and in 33% of children in a Canadian series. [5] Thrombosis is associated with a central venous catheter in 80% of newborns and 50% of children with upper extremity thrombosis. [6]
According to a study by Sandoval et al, the incidence of clinically evident DVT in hospitalized children increased from 0.3 cases to 28.8 cases per 10,000 hospital admissions between 1992 and 2005, with central venous catheters accounting for 45% of DVTs that developed during the patient’s hospital stay (vs those that were already present on admission). [7]
Antiphospholipid antibody syndrome
Antiphospholipid antibodies, which are detected by finding positive lupus anticoagulant or anticardiolipin antibodies, are associated with thrombosis in adults and children. In 2 studies of children with systemic lupus erythematosus and associated anticardiolipin antibodies, the incidences of thromboembolism were 9.2% and 17%. However, most children with antiphospholipid antibody syndrome acquire it incidentally and do not have systemic lupus erythematosus.
In one study, in which 95 children with lupus anticoagulant were followed for a median of 5.3 years, bleeding symptoms were found in approximately 10% of these children, while 5% had a thrombotic event.
Disseminated intravascular coagulation
Sepsis and disseminated intravascular coagulation have been associated with thromboembolism in children and in adults. Microvascular thrombosis consumes clotting factors, predisposing the patient to hemorrhage and thromboembolism. Treatment of the underlying cause is essential.
Surgery, immobilization, and prolonged bedrest
The effects of surgery, immobilization, and prolonged bed rest on thromboembolism risk have been studied extensively in adults, and evidence-based recommendations for prophylaxis against thromboembolism have been widely disseminated.
Compared with adults, children have a much lower risk of thrombosis after surgery. Therefore, prophylactic administration of heparin or low-molecular-weight heparin (LMWH) is not recommended for children unless additional risk factors are present (eg, obesity, oral contraceptive use, cancer, central venous catheter). [8]
Malignancy
Malignancy-associated thromboembolism has been studied most extensively in children with acute lymphoblastic leukemia. The underlying mechanisms are complex and include the effect of leukemia itself and the use of chemotherapy, especially treatment with L-asparaginase. In addition, permanent central venous catheters are placed in many children with malignancies.
A Canadian study, by Pelland-Marcotte et al, reported that in patients below age 15 years with hematologic malignancy, risk factors for the development of thromboembolism include age less than 1 year, age 5-9.99 years, or age 10-14.99 years; hematopoietic stem cell transplantation; anthracyclines; and asparaginase. In children under age 15 years with solid tumors, thromboembolism risk factors include obesity, surgical treatment, radiotherapy, anthracyclines, and platinum drugs. [9]
Use of estrogen-containing medications
Oral contraceptives, especially those that contain estrogen, are associated with a 4-fold increase in the risk of venous thrombosis and a 22-fold increase in the risk of cerebral thrombosis. This risk may be explained by the acquisition of resistance to activated protein C. Administration of oral contraceptives to patients who are heterozygous for the factor V Leiden mutation increases the risk of venous thromboembolism 35-fold to 50-fold. In women with antithrombin, protein C, or protein S deficiency who are taking oral contraceptives, the risk rises 6-fold.
However, the absolute risk is only 0.3% per year, and pregnancy itself produces a prothrombotic state; thus, benefits must be weighed against risks when helping patients to decide whether or not to use contraceptives and which method to choose.
Nephrotic syndrome
Children with proteinuria at levels of more than 0.5 g/day may have a loss of anticoagulant proteins (eg, antithrombin), which increases the risk of thromboembolism. Most thromboembolisms develop within several months of diagnosis. Arterial thromboembolism and venous thromboembolism can occur; renal vein thrombosis is most common.
Heparin-induced thrombocytopenia
Heparin-induced thrombocytopenia is characterized by a decrease of more than 50% in the platelet count from the base line after a patient is given unfractionated heparin for 5 days or longer; this is less common in patients treated with LMWH.
Heparin-induced thrombocytopenia can be complicated by venous and arterial thrombosis, so a high index of suspicion is needed to recognize this syndrome in children, including those who are receiving only heparin flushes to maintain the patency of intravenous or central lines. Management includes cessation of all forms of heparin and administration of a direct thrombin inhibitor until the platelet count normalizes and the patient can be transitioned to warfarin anticoagulation.
Inherited prothrombotic disorders
Several dominantly inherited deficiencies or abnormalities of proteins involved in the coagulation and fibrinolytic pathways are now recognized. Occasionally, more than 1 such abnormality may coexist in a single patient. The risk of venous thromboembolism in patients with these abnormalities depends not only on the number of concomitant inherited risk factors but also on the number of acquired risk factors such as orthopedic surgery or trauma, immobility, pregnancy, use of oral contraceptives, and dehydration.
Factor V Leiden
Resistance to activated protein C due to a point mutation in factor V (named factor V Leiden, after the city in which the discovery was made) is the most common genetic risk factor associated with venous thrombosis in adults and children. This mutation prevents cleavage of activated factor V Leiden by activated protein C and thus promotes ongoing clot development.
Approximately 3-8% of whites are heterozygous for the mutation, but many have no history of thrombosis. Several pediatric studies have demonstrated that 10-50% of children with thrombosis are heterozygous for the factor V Leiden mutation. Heterozygous factor V Leiden mutation is associated with a seven-fold increase in the incidence of thrombosis.
Double heterozygotes for factor V Leiden and for protein C, protein S, or antithrombin deficiency have been reported; these individuals have a further increase in their risk of thrombosis.
Among women who are heterozygous for factor V Leiden who also are taking oral contraceptives, the risk of thrombosis rises 35-fold. Even so, very few develop thrombosis during adolescence, and usually only do so when additional risk factors are present.
Antithrombin deficiency
Produced in the liver, antithrombin is the most important inhibitor of activated clotting factors. Most patients with antithrombin deficiency are heterozygous (with levels < 50%), and thrombosis in this population is usually venous. Thrombosis can occur in children as young as 10 years.
Homozygous deficiency of antithrombin is rare but devastating. Patients usually present within hours of birth and have extensive thrombosis. Most infants die soon after birth.
Protein C deficiency
Protein C deficiency is usually transmitted in an autosomal dominant manner with incomplete penetrance. Thrombosis occurring in association with protein C deficiency is most often venous and in the lower extremities. DVT in heterozygotes can be observed as early as the teenage years. Similar to homozygotes with antithrombin deficiency, homozygotes with protein C deficiency usually present in the newborn period, with purpura fulminans. A purified protein C concentrate (Ceprotin) has been designated as an orphan drug for the treatment of protein C deficiency.
Patients with either protein C or protein S deficiency (both are vitamin-K dependent) who require anticoagulation can develop warfarin-induced skin necrosis unless heparin is started first.
Protein S deficiency
Protein S deficiency is similar to protein C deficiency and antithrombin deficiency, except that it enhances an individual's predisposition to develop arterial thrombosis. Most protein S is bound to C4-binding protein. Therefore, one must measure both free and total concentrations of protein S to rule out a deficiency, even though the free protein S is the one that plays a role as anticoagulant.
As stated above, warfarin-induced skin necrosis can occur in patients with either protein C or protein S deficiency who require anticoagulation, unless heparin is started first.
Hyperhomocysteinemia
In adults, hyperhomocysteinemia is an independent risk factor for arterial vascular disease and venous thrombosis. A study of 45 children with ischemic stroke demonstrated that their odds ratio for moderate hyperhomocysteinemia, in comparison with control subjects, was 4.4, indicating that it is a risk factor for pediatric venous thrombosis as well.
A German study of 163 children with venous thromboembolism showed a 3-fold increase in the risk for this condition among subjects with elevated fasting homocysteine levels. [10] Homozygous mutations in the gene for cystathionine beta synthetase, although rare, account for most cases of severe hyperhomocysteinemia.
Mild to moderate hyperhomocysteinemia can occur in heterozygotes with mutations affecting cystathionine beta synthetase or methylene tetrahydrofolate reductase.
Prothrombin gene 20210A mutation
A Turkish study of 32 children with cerebral infarcts revealed that 21.8% were heterozygous for the prothrombin gene 20210A mutation. [11] Studies have shown that this mutation increases the risk for pediatric arterial thrombosis, especially in the central nervous system (CNS).
Elevated lipoprotein(a) levels
Elevated lipoprotein(a) levels have been found in children with thromboembolism. Other disorders, such as dysfibrinogenemia and plasminogen deficiency, are rare but should be evaluated for if the rest of the workup yields negative results.
Factors VIII and XI
Studies in adults have implicated elevated levels of factor VIII and factor XI as risk factors for thrombosis, but whether they are risk factors in children is unknown.
Congenital heart disease
Congenital heart disease can be a thromboembolic risk factor for children with mechanical or prosthetic valves and for those undergoing Blalock-Taussig shunt placement or a Fontan procedure. As noted above, cardiac catheterization is the most common risk factor for arterial thrombosis.
Cardiogenic embolism due to atrial fibrillation or cardiomyopathy is a cause of stroke in children and adults.
A study by Yamamura et al suggested that in patients with concurrent congenital heart disease and asplenia, thromboembolism is more likely to develop during management of the disease than it is in patients who have congenital heart disease but are not asplenic. The study involved 161 patients with congenital heart disease who underwent cardiac catheterization; 46 of the patients had asplenia, and 115 patients did not. [12]
The investigators found that, unlike the patients without asplenia, those who were asplenic had persistent thrombocytosis. There was also a higher incidence of thromboembolic complications in the asplenic patients than in the nonasplenic group (28% vs 10%, respectively). The finding emphasizes the fact that in children, usually multiple risk factors must be present to lead to a significant incidence of thrombosis.
Epidemiology
Occurrence in the United States
The rate of venous thromboembolism in pediatric tertiary care hospitals reportedly underwent a significant increase between 2001 and 2007. A study by Raffini et al found that the annual rate grew from 34 to 58 cases per 10,000 hospital admissions, a rise of 70%. According to the report, the increased rate encompassed newborns, infants, children, and adolescents. [13, 14]
International occurrence
In a German study, by Nowak-Gottl et al, the incidence of symptomatic neonatal thromboembolism was 5.1 cases per 100,000 births. [15]
In the aforementioned Canadian study by Pelland-Marcotte et al, the investigators reported that a clinically significant thromboembolism developed in 4% of children under age 15 years with cancer, as calculated using a population-based cohort. [9]
Race-, sex-, and age-related demographics
Although some prothrombotic risk factors are more common in particular racial groups, overall there is no evidence to suggest that children of any particular race are at higher risk for thromboembolism. With regard to sex predilection, male and female children are equally affected by thromboembolism.
The incidence of thromboembolism peaks in newborns and infants younger than 1 year, then remains very low until adolescence, when the incidence begins to increase. [13]
Prognosis
Potential complications of thromboembolism include the following:
-
Recurrent thrombosis
-
Pulmonary embolism
-
Postthrombotic syndrome
-
Bleeding
-
Death
Many children with thromboembolism have a persistent underlying risk factor, such as congenital heart disease.
Recurrent thromboembolism
Recurrence may occur secondary to inadequate anticoagulation because of a concern about bleeding and/or the persistence of underlying risk factors, such as the use of a central venous catheter.
A German study showed that a number of underlying genetic risk factors affected recurrence rates. Children with no genetic risk factors had a 4.8% recurrence rate, whereas those with 1 genetic risk factor had a 17.6% recurrence rate. In children with 2 or more genetic risk factors, the risk of recurrence was almost 50%.
Goldenberg et al noted an increased recurrence rate in children with venous thromboembolism and elevated levels of factor VIII and/or D-dimer after 3-6 months of anticoagulation therapy. [16]
Postthrombotic syndrome
Postthrombotic syndrome consists of chronically swollen, painful extremities with induration of the skin, ulceration, and pigmentary changes secondary to chronic venous stasis. From 20-67% of adults with DVT develop postthrombotic syndrome, while the Canadian registry of pediatric DVT and PE documented the syndrome in 21-25% of children with venous thrombosis. [17, 18]
Using a standardized score, investigators in a study from the Hospital for Sick Children in Toronto, Canada, observed postthrombotic syndrome in 63% of 153 children. Cases were mild in 83% and moderate in 17%. [19] The mild cases, which were detected only by use of prospective observation using a standard methodology and trained personnel, would be unlikely to appear in the registry cited above, which explains the apparently discrepant results.
Treatment of postthrombotic syndrome consists of the use of elastic compression stockings, elevation of the extremity above the level of the heart, and administration of analgesics or narcotics as necessary.
-
Virchow triad for the pathophysiology of thrombus formation.
-
Coagulation cascade. Solid arrows represent activation events, dashed arrows represent inhibition events, and dotted lines with circles represent inactivation events. a = active; APC = activated protein C; F = factor; FDP= fibrin degradation products; HMW = high molecular weight; PAI-1 = plasminogen activator inhibitor-1; PL = phospholipid; TM = thrombomodulin; t-PA = tissue type plasminogen activator; u-PA = urokinase plasminogen activator; XL= crosslinked.
-
Nomogram for adjusting the dosage of heparin. Reproduced with permission from Michelson et al (1998). APTT = activated partial thromboplastin time.
-
Dosing of low-molecular-weight heparins (LMWHs) in children. Reproduced with permission from Michelson et al (1998).
-
Warfarin dosing in children. INR = international normalized ratio. Reproduced with permission from Michelson et al (1998).
-
The pathophysiology of pulmonary embolism. Although pulmonary embolism can arise from anywhere in the body, most commonly it arises from the calf veins. The venous thrombi predominately originate in venous valve pockets (inset) and at other sites of presumed venous stasis. To reach the lungs, thromboemboli travel through the right side of the heart. RA, right atrium; RV, right ventricle; LA, left atrium; LV, left ventricle.
-
Axial CT scan of thorax shows an embolus in the distal left pulmonary artery with an associated pleural effusion.
-
Thrombosis and thrombophilia.







