Practice Essentials
Of the 32 recognized species of Taenia, only Taenia solium (pork tapeworm) and Taenia saginata (beef tapeworm) are medically important. However, epidemiologic studies in Southeast Asia have identified a third Taenia species in humans, known as Taenia asiatica. [1, 2]
Taeniasis is an infection due to an adult tapeworm in the intestine. Humans acquire taeniasis from ingestion of undercooked pork containing cysticerci. Cysticercosis is the development of extraintestinal encysted larval forms of T solium in various organs. Humans develop cysticercosis from ingestion of T solium egg excreted by themselves (autoinfection), or by a human tapeworm carrier, which means humans can have cysticercosis even though they do not eat pork (see Cysticercosis). The CNS is involved in 60-90% of cases; this condition is termed neurocysticercosis (NCC). [3] See the image below. For more information, see Neurocysticercosis.
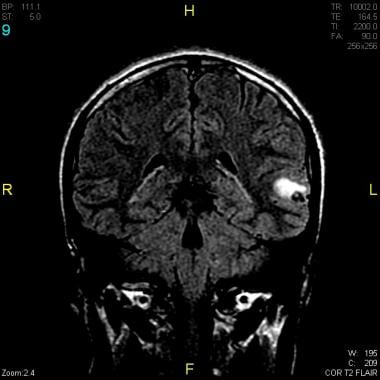 Brain MRI that reveals a cystic lesion containing a dead parasite with surrounding vasogenic edema on fluid-attenuated inversion recovery (FLAIR) imaging. MRI is of a 16-year-old Guatemalan adolescent with first-time afebrile seizure and normal EEG, cerebrospinal fluid (CSF), and examination findings.
Brain MRI that reveals a cystic lesion containing a dead parasite with surrounding vasogenic edema on fluid-attenuated inversion recovery (FLAIR) imaging. MRI is of a 16-year-old Guatemalan adolescent with first-time afebrile seizure and normal EEG, cerebrospinal fluid (CSF), and examination findings.
Differentiating between T solium and T saginata infections is important because infection with T solium can cause neurocysticercosis, which is one of the leading cause of deaths from food-borne illnesses, resulting in a total of 2.8 million disability-adjusted life-years (DALYs) according to the World Health Organization (WHO). [4] Cysticercosis caused by T saginata is rare; T saginata has far lower impact on human health than T solium. Both infections are endemic in Southeast Asia, Africa, Europe, and Central and South America. Infection in children usually goes unrecognized. [5] WHO developed a roadmap for control and eradication of T solium taeniasis/cysticercosis to be implemented in selected countries. [4]
Signs and symptoms
Most persons with taeniasis are either asymptomatic or have mild to moderate complaints.
The most common complaint is passage (active or passive) of proglottids, which is associated with slight discomfort. Other symptoms include the following:
-
Colicky abdominal pain (more common in children)
-
Nausea
-
Weakness
-
Loss of appetite
-
Increased appetite
-
Headache
-
Constipation
-
Dizziness
-
Diarrhea
-
Pruritus ani
-
Hyperexcitability
See Presentation for more detail.
Diagnosis
A complete blood cell (CBC) count detects mild eosinophilia.
Examine three stool samples (direct and concentrated stool preparations) collected on 3 different days from patients and contacts.
Copro-Ag enzyme-linked immunosorbent assay (ELISA) can be used to detect T solium tapeworm carrier with a sensitivity of 84.5% and a specificity of 92%.
Computed tomography (CT) is superior to magnetic resonance imaging (MRI) for the detection of intracerebral calcification. Note that calcification occurs less frequently in children than in adults.
See Workup for more detail.
Management
Most patients with intestinal Taenia infection are asymptomatic or mildly symptomatic. If adult tapeworms are detected in the stools, anthelmintic therapy usually suffices.
See Treatment and Medication for more detail.
Patient education
Educate patients and families about routes of infection and preventive measures.
Teach patients and families proper sanitary and personal hygiene measures.
Pathophysiology
Humans are the definitive host. Adult tapeworms live in the human small intestine. Humans pass gravid eggs in feces; these mature eggs contaminate pastures and barnyards, where cattle and pigs ingest them. Upon reaching the alimentary canal of infected animals, the embryos are released, penetrate the gut wall, and enter the circulation. The embryos filter from the circulation and encyst in muscular tissue. Larvae (ie, cysticerci) become infectious within 2-3 months. Humans develop a tapeworm infection by eating raw or undercooked beef or pork containing cysticerci. The cysticercus becomes activated, attaches to the wall of the small intestine by the scolex, and becomes a mature tapeworm. This maturation process takes 10-12 weeks for T saginata and 5-12 weeks for T solium. A single tapeworm produces an average of 50,000 eggs per day and may live up to 25 years.
Pigs are the intermediate host for T solium and T asiatica. The larvae of T solium have predilection to infect the muscles and brain of pigs; however, the larvae of T asiatica tend to infect pig viscera, especially pig liver. Cows are the intermediate host for T saginata with the larvae predominantly found in the muscle.
Humans can also act as an intermediate host for T solium. Cysticercosis results from human ingestion of T solium eggs through fecal contamination, reverse peristalsis of gravid proglottids, or autoinfection. The cysticerci may develop in any organ, and their effects depend entirely on the location of the cysticerci.
A coenurus is the larval stage of Taenia multiceps, Taenia serialis, and Taenia brauni. Adult tapeworms develop in dogs or other canids that ingest coenurus larvae in the tissues of various intermediate hosts. These hosts include sheep, goats, hares, rabbits, and other herbivores for T multiceps; hares, rabbits, and other rodents for T serialis; and gerbils for T brauni. Each protoscolex within a coenurus can mature into an adult tapeworm after ingestion by a canid host. Adult worms produce eggs, which are passed in feces; these eggs are morphologically similar to taeniid eggs. Ingestion of eggs by an appropriate intermediate host or by humans leads to development of coenurus. Coenuri are cysts that contain many protoscolices attached in rows on the internal membrane of the cyst.
Etiology
Taeniasis is caused by ingesting inadequately cooked beef or pork that contains the larvae or cysticerci of T saginata or T solium respectively. Cysticercosis, which is caused by ingesting eggs of T solium, occurs when larvae are deposited in skeletal muscle, brain, eyes, and other organs. Taeniasis is endemic in countries where both T saginata and T solium are common and public hygiene is poor.
T asiatica, a species of Taenia identified in many Southeast Asian countries, resembles T saginata at morphology of adult worms and larvae but different at the molecular level, and its ingestion in inadequately cooked pork or pork viscera, especially pork liver, causes an intestinal infection. This close relationship with T saginata has led to the assumption that it does not cause human cysticercosis because human cysticercosis is caused almost exclusively by T solium.
Coenurosis results when humans accidentally ingest mature T multiceps or T serialis eggs, usually in contaminated fruits or vegetables. Approximately 100 cases of coenurosis have been reported, primarily in tropical Africa, with the remainder in North and South America and South Africa. Interestingly, the cases in central Africa rarely involved the CNS, whereas more than 75% of the cases elsewhere had CNS involvement. Larvae of these species may be inoculated directly into a child's conjunctiva and skin as the child plays on contaminated ground.
Epidemiology
United States statistics
Cysticercosis is primarily an imported disease. Approximately 1000 cases are diagnosed each year. Most occur in persons who have immigrated, primarily from Latin America. [6] Cysticercosis has also developed following close contact with recently immigrated, infected individuals. Although some patients with NCC are born in the United States, many have traveled to rural areas in countries where the condition is endemic. Locally acquired infections have been confirmed in Los Angeles, New York, Chicago, Oregon, [7, 8] and elsewhere. Although T saginata infection occurs worldwide, prevalence in the United States is less than 1% because most US cattle are free of the parasite.
A study analyzed in-patient records using the Nationwide Inpatient Sample for 1998-2011 to estimate cysticercosis-related hospitalizations and patient/institutional characteristics in the United States. The study reported that there were an estimated 33,060 cysticercosis-related hospitalizations nationwide, representing a hospitalization rate of 8.03 per million population. The study further reported that the highest proportion of cases were male (54.8%), Hispanic (62.0%), aged 18-44 (58.8%), and occurred in the West (45.1%). An estimated 459 deaths occurred, representing an in-hospital case-fatality rate of 1.4%. [9]
International statistics
Approximately 50 million people worldwide are infected by T saginata or T solium. Approximately 50,000 people die annually of cysticercosis. T saginata is common in cattle-breeding regions. Areas with the highest (ie, >10%) prevalence are central Asia, the Near East, and central and eastern Africa. [10, 11, 12] Areas with low (ie, 1%) prevalence are Southeast Asia, Europe, and Central and South America. A systematic review of the geographical distribution of T saginata throughout Asia found that the only country that reported its absence was Japan. [13]
T solium is endemic in Central and South America, Southeast Asia, [14, 15, 16] India, the Philippines, Africa, [17] Eastern Europe, and China. Areas of highest prevalence include Latin America and Africa. In some regions of Mexico, prevalence may reach 3.6% of the general population.
A study of school-aged children from 27 schools in China showed overall prevalence of T solium cysticercosis to be 6%. In three schools the prevalence was 15% or more. Risk factors for cysticercosis included pig ownership, feeding pigs with human feces, and worms in their feces. Schools with higher prevalence had more students with households that have free-range pigs and practice open defecation. [18]
A meta-analysis of studies on the distribution of Taenia infections in India demonstrated that the prevalence of T solium taeniasis/cysticercosis was 11.06% and the prevalence of T saginata taeniasis was 4.7%. [19]
T multiceps has been reported in the Americas and parts of Europe and Africa.
T serialis infections occur in the United States and Canada.
T brauni has been reported in Africa.
Race-, sex-, and age-related demographics
Race
All races are equally affected.
Sex
Both genders are equally affected.
Age
All ages are susceptible to infection. The age at which raw meat consumption begins is the primary determinant. T solium taeniasis has been reported in children older than 2 years in certain rural communities of Mexico.
Prognosis
Treatment with praziquantel reportedly provides cure rates of 99-100%.
Morbidity/mortality
Most intestinal taeniid infections are asymptomatic. When symptoms occur, they are usually mild and involve abdominal pain, anorexia, weight loss, or malaise. Cysticercosis causes a mass effect in various vital organs (eg, brain, eye, heart). The mortality rate for cysticercosis is low and is generally caused by complications such as encephalitis, increased intracranial pressure secondary to edema and/or hydrocephalus, and stroke.
Complications
Complications include the following:
-
Appendicitis
-
Cholecystitis
-
Pancreatitis
-
Intestinal obstruction
-
Tubo-ovarian abscess (rare)
-
Systemic cysticercosis [20]
-
Brain MRI that reveals a cystic lesion containing a dead parasite with surrounding vasogenic edema on fluid-attenuated inversion recovery (FLAIR) imaging. MRI is of a 16-year-old Guatemalan adolescent with first-time afebrile seizure and normal EEG, cerebrospinal fluid (CSF), and examination findings.





