Background
Congenital sinus of Valsalva aneurysm [1] was first described by Hope in 1839. [2] This first published account describes rupture of a sinus of Valsalva, which is the most feared complication. Soon afterwards, clinicians described other cases of unruptured aneurysms and applied anatomic descriptions. The condition may have been clinically described for the first time in 1883. [2]
The three sinuses of Valsalva are located in the most proximal portion of the aorta, just above the cusps of the aortic valve. The sinuses correspond to the individual cusps of the aortic valve. These structures contained within the pericardium are easily revealed using aortography and echocardiography as distinct but subtle out-pouchings of the aortic wall just above the valve. The sinuses end in the area of the sinotubular junction, where the tubular portion of the aorta begins.
Aneurysm of a sinus of Valsalva is a rare congenital cardiac defect that can rupture, causing heart failure or other catastrophic cardiac events. If the aneurysm remains unruptured, it occasionally causes obstruction of cardiac flow resulting from compression of normal structures. Dissection of the aneurysm into the cardiac tissues may occur, causing obstruction or destruction of local structures.
Acquired aneurysmal dilatation of the sinuses of Valsalva may occur because of Marfan syndrome, syphilitic aortitis, or as a function of aging. These entities are not discussed in this article. See the image below.
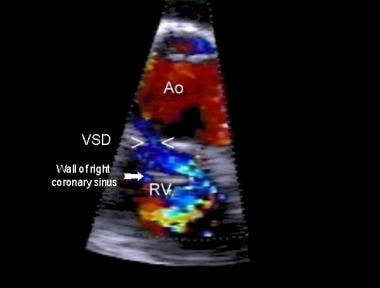 Sinus of Valsalva aneurysm. Color-flow Doppler ultrasonography is performed in the right ventricle through a supracristal ventricular septal defect with fingerlike prolapse of the right coronary sinus wall (arrow).
Sinus of Valsalva aneurysm. Color-flow Doppler ultrasonography is performed in the right ventricle through a supracristal ventricular septal defect with fingerlike prolapse of the right coronary sinus wall (arrow).
Pathophysiology
Aneurysmal dilatation of the sinuses of Valsalva occurs when the aortic media is defective, allowing separation of the media from the aortic annulus fibrosus. [3] The defect is inherited, but frank aneurysmal dilatation is rarely seen at birth. Sinus of Valsalva aneurysm is associated with a ventricular septal defect in approximately 40% of patients.
Aneurysms typically develop as a discrete flaw in the aortic media within one of the sinuses of Valsalva. Aneurysms most often involve the right aortic sinus (67-85% of patients, often associated with a supracristal ventricular septal defect), followed by the noncoronary sinus, whereas an aneurysm of the left sinus is rare. [3] Under the strain of aortic pressure, the sinus gradually weakens and dilates, causing the formation of an aneurysm. Lack of supporting tissue (eg, ventricular septal defect) may contribute to instability and progressive distortion of the aortic sinus, often with associated aortic insufficiency. Deficiency of the aortic media where it attaches to the aortic annulus produces dilation of the aortic sinuses, usually over many years.
Distortion and prolapse of the sinus and aortic valve tissue can lead to progressive aortic valve insufficiency. Unruptured aneurysm may cause distortion and obstruction in the right ventricular outflow tract. Distortion and compression may also cause myocardial ischemia (by coronary artery compression) and, possibly, heart block (by compressing the conduction system). Rupture may occur into any chamber, although rupture most commonly occurs into the right ventricle resulting in aortic right ventricular communication. Rupture into the right atrium is the second most common, in association with a noncoronary cusp aneurysm. Rupture may occur less commonly into the left-sided chambers, [4] the pulmonary artery, [5, 6] and rarely extends into the pericardium.
Etiology
Sinus of Valsalva aneurysm is presumed to be caused by a spontaneous genetic mutation. Although the defect is inherited, no distinct pattern of inheritance has been noted. Frank aneurysmal dilatation is rarely seen at birth.
Subpulmonic ventricular septal defect may be an important contributing factor in the progression of sinus of Valsalva aneurysms.
Tertiary syphilis is of historical significance as a cause for aortic aneurysms.
Traumatic injury to the aortic root (usually from direct chest compression) may rarely cause rupture of the aortic root.
A number of generalized disorders may be associated with dilatation and/or distortion of the aortic root, including Marfan syndrome, Ehlers-Danlos syndrome, Turner syndrome, Williams syndrome, bicuspid aortic valve, and osteogenesis imperfecta.
Epidemiology
United States data
Sinus of Valsalva aneurysm comprises approximately 0.1-3.5% of all congenital cardiac anomalies. Discovery in the pediatric age group is unusual.
International data
Incidence in the Western Hemisphere (outside of the United States) is approximately the same as in the United States. An increase in prevalence is observed in Asians because of the higher incidence of supracristal (subpulmonic) ventricular septal defects.
Race-, sex-, and age-related demographics
Increased incidence in the Asian population has been described, which is secondary to increased incidence of supracristal ventricular septal defect in Asians. These ventricular defects may contribute to instability of the aortic sinuses, particularly the right aortic sinus.
Male-to-female ratio is 4:1.
Average age of patients with rupture of a sinus of Valsalva aneurysm is approximately 30 years, with a range of 11-67 years in one series. [7] Problems in infancy and early childhood are uncommon but have been reported. [8, 9]
Prognosis
Prognosis after surgical repair in patients with sinus of Valsalva aneurysm is excellent, particularly if the aortic valve has not been damaged. [10] Prognosis in patients with a ruptured aneurysm who have not undergone surgical repair may be poor, with survival beyond 1 year uncommon. [11, 12, 10]
Prognosis in patients with an unruptured sinus of Valsalva aneurysm is unknown because patients may be entirely asymptomatic.
In a retrospective review of 255 Chinese patients who underwent surgical repair of congenital sinus of Valsalva aneurysm over a 7-year period, investigators indicated good outcomes, but the presence of aortic regurgitation at discharge is an independent risk factor for exacerbation of aortic regurgitation at late follow-up. [13] The origin of the aneurysm in 212 patients (83.1%) was the right sinus, and in 38 patients (14.9%), it was the noncoronary sinus. Of 142 patients (55.7%) who had aortic regurgitation, 60 received aortic valve replacement and 13 received aortic valvuloplasty. Three of the valvuloplasties failed and the affected patients underwent aortic valve replacement.
Risk factors for aortic valve regurgitation included the presence of infective endocarditis, the presence of a nonruptured sinus of Valsalva aneurysm, and the cardiothoracic ratio. There were no early deaths reported, but there were two late deaths and two patients with complications associated with anticoagulation. Of 150 patients who had late follow-up, echocardiography showed 17 had improvement of aortic regurgitation, whereas progression occurred in 20. [13]
Morbidity/mortality
Morbidity and mortality are most often associated with acute severe aortic valve insufficiency resulting from aneurysm rupture. The mortality rate in patients with a sinus of Valsalva aneurysm in whom surgery is not performed is high within the first year after rupture. [3, 11, 14]
Causes of sudden death from sinus of Valsalva aneurysm most commonly involve rupture of the aneurysm with the acute onset of overwhelming congestive heart failure, cardiac tamponade, dysrhythmia, or coronary ischemia, depending on the location of the aneurysm and the subsequent flow disturbance. Size and location of the shunt are the major determinants of presentation and prognosis. Late death usually occurs within 1 year after rupture if the shunt is substantial; longer survival may occur if the shunt is small. [12, 14]
Major cardiac morbidity and late mortality in this condition also depend on the magnitude and location of shunts. In some instances, an unruptured aneurysm also causes major symptoms and hemodynamic alterations because of obstruction of valves or impingement upon cardiac structures (eg, coronary arteries, conduction system).
The surgical mortality rate is estimated to be 5% or less.
Complications
The following complications may arise in patients with sinus of Valsalva aneurysm:
-
Congestive heart failure with acute or progressive rupture or with aortic valve insufficiency
-
Infective endocarditis (possibly associated with smaller ruptured aneurysms in 5-10% of patients) [15]
-
Angina and myocardial ischemia
-
Heart block resulting from compression of the conduction system [16]
-
Aortobronchial fistula or aortopulmonary artery fistula (possible rare complications)
-
Abnormal flow (spontaneous contrast) in a dilated unruptured sinus of Valsalva aneurysm (postulated to be a source for systemic embolization)
Patient Education
Educate parents of pediatric patients with sinus of Valsalva aneurysm regarding avoidance of contact sports and strenuous activities, especially heavy lifting.
For patient education resources, see Aortic Aneurysm.
-
Sinus of Valsalva aneurysm. Color-flow Doppler ultrasonography is performed in the right ventricle through a supracristal ventricular septal defect with fingerlike prolapse of the right coronary sinus wall (arrow).
-
Sinus of Valsalva aneurysm. Apical four chamber (left) and precordial short axis (right) views demonstrating aneurysm (ANU) of the sinus of Valsalva protruding from the aorta (Ao). LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; TV, tricuspid valve.
-
Sinus of Valsalva aneurysm. Selected frame from aortic (Ao) root cineangiography following coil occlusion demonstrating complete ablation of the shunt. ANU, aneurysm; R, rupture; RV, right ventricle.








