Practice Essentials
Right middle lobe syndrome (RMLS) generally refers to chronic or recurrent atelectasis in the right middle lobe of the lung. First described in the medical literature in 1948, [1] it is caused by various etiologies and has no consistent clinical definition. Right middle lobe syndrome is characterized by a wedge-shaped density that extends anteriorly and inferiorly from the hilum of the lung, which is best visualized using lateral chest radiography.
See the image below.
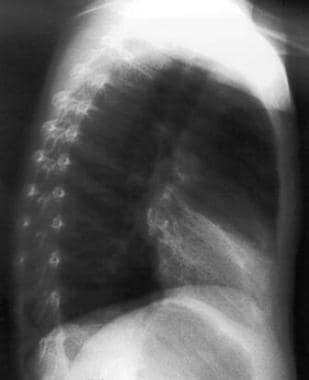 Lateral view chest radiograph showing a wedge-shaped density extending from the hilum anteriorly and inferiorly.
Lateral view chest radiograph showing a wedge-shaped density extending from the hilum anteriorly and inferiorly.
This condition is most common in children with a history of asthma or atopy. Although the mechanism by which asthma leads to lobar atelectasis is unknown, associated inflammation, bronchospasm, and secretions that cause mucus plugging are likely major contributors. Management is determined by etiology, and most patients respond to medical therapy alone.
Pathophysiology
Certain anatomical characteristics make the right middle lobe susceptible to transient obstruction as a result of inflammation or edema. The narrow diameter of the lobar bronchus and acute take-off angle create poor conditions for drainage. Relative anatomical isolation of the middle lobe and poor collateral ventilation decrease the chance of reinflation once atelectasis occurs. Bronchial obstruction can result from extrinsic compression as in hilar lymphadenopathy or tumor of neoplastic origin; however, atelectasis in children usually results from a process such as asthma-associated edema and inflammation. Foreign body aspiration into the right middle lobe orifice can also predispose to collapse of the lobe.
Etiology
Intra-airway origin
In children, right middle lobe syndrome is usually secondary to primary ventilation disorders. Chronic inflammation of the airways, which contributes to atelectasis of the right middle lobe, is present. A paucity of collateral ventilation is observed in children and serves to prevent reinflation.
Primary disorders of ventilation include the following:
-
Asthma
-
Chronic pneumonia or bronchitis
-
Other chronic lung diseases caused by aspiration or gastroesophageal reflux
-
Primary ciliary dyskinesia (immotile cilia syndrome)
-
Airway foreign body aspiration
-
Endobronchial tumors
-
Mucus plugging, as from any of the above
-
Granulation tissue
Extra-airway origin
Extraluminal compression is caused by the following:
-
Cardiovascular anomalies
-
Congenital malformations such as situs inversus and other anatomical defects such as anomalous branching or abnormal diameter, length, or structure of the bronchi
-
Lymphadenopathy of peribronchial nodes
-
Tumors
-
Traction diverticula of the esophagus
Infectious etiologies
Whether the infection is a cause of the collapse or a result of airway stasis and poor clearance may not be clear. Primary infectious etiology is more frequent in adults; however, one pediatric study found that 50% of children with collapsed right middle lobe had an underlying bacterial infection. [2] Infectious causes also increase in frequency among immunocompromised patients.
Common bacterial causes in children include Streptococcus pneumoniae and Haemophilus influenzae.
Fungal causes include histoplasmosis, blastomycosis, and aspergillosis, which manifest as allergic bronchopulmonary aspergillosis (APBA).
Mycobacteria, including Mycobacterium tuberculosis, Mycobacterium avium-intracellulare, and Mycobacterium fortuitum have also been identified as causal agents.
Occurrence is mainly caused by extrinsic compression by hilar lymph nodes, which are commonly observed in these infections as well as in fungal infections.
Epidemiology
United States statistics
The precise incidence in children is unknown. Right middle lobe syndrome is widely underdiagnosed and frequently unrecognized.
Sex- and age-related demographics
Right middle lobe syndrome has been said to occur twice as often in girls than in boys; however, large epidemiologic studies are lacking.
Symptoms begin in early childhood, usually in children aged 1-2 years. Symptom frequency decreases in later childhood, but the interval between onset of symptoms and diagnosis widely varies.
Prognosis
Historically, right middle lobe syndrome has been reported to resolve in approximately 33% of children after bronchoscopy. Approximately 33% recover eventually with medical management, 22% require lobectomy, and 11% have decreased severity of symptoms but should be monitored for the possibility of requiring lobectomy later. While recent published data are lacking, with aggressive modern therapy as outlined above, it is more likely that the number of patients requiring lobectomy is far lower. In our own experience spanning 30 years, lobectomy was performed only once due to frequent recurrent pulmonary infections and failure to gain weight.
About one third of patients with right middle lobe syndrome in early childhood continue to have symptoms in later childhood. These patients usually experience asthma symptoms or another chronic lung condition such as cystic fibrosis. A study examined the efficacy of early postnatal corticosteroids for preventing chronic lung disease in preterm infants. [3]
The remaining two thirds of children with right middle lobe syndrome do not have persistent symptoms later in adulthood.
Morbidity/mortality
Severity in children ranges from mild atelectasis and scarring of no consequence to severe bronchiectasis requiring surgical resection, although this has become a rarity in the modern era.
Complications
Long-term complications range from none to minimal pulmonary scarring of no discernible physiological consequence to severe bronchiectasis requiring surgical intervention.
In children with asthma, right middle lobe syndrome may produce a vicious cycle of infection, inflammation, and asthma exacerbation.
A retrospective study by Feng et al found that asthmatic children with recurrent middle lobe syndrome had more frequent episodes of severe asthma and severe exacerbations than did asthmatic children with transient middle lobe syndrome. [4]
Patient Education
Because chest physical therapy and postural drainage are of paramount importance in the management of RMLS, instruct the caretaker with appropriate techniques and position for right middle lobe physiotherapy. This is often performed by a registered respiratory or physical therapist. Regardless, the therapist should be somebody who frequently deals with children.
Flutter valve and high-frequency oscillation (known as the vest) have not been studied in this setting, but they may be alternative modalities of delivering chest physical therapy.
-
Posterioranterior chest radiograph demonstrating right middle lobe infiltrate in a 9-year-old male with a history of severe asthma. Note the blurred right heart border.
-
Lateral view chest radiograph in a 9-year-old male with severe asthma showing a wedge-shaped density extending from the hilum anteriorly and inferiorly.
-
High-resolution chest CT showing marked chronic changes and volume loss in the right middle lobe with diffuse traction bronchiectasis in 9-year-old male with a history of severe asthma and RML syndrome.
-
Posteroanterior chest radiograph demonstrating right middle lobe collapse and infiltrate. Note blurred right heart border.
-
Lateral view chest radiograph showing a wedge-shaped density extending from the hilum anteriorly and inferiorly.
-
Chest CT scan showing extensive bronchiectasis of both medial and lateral segments of the right middle lobe.








