Overview
Obesity is a growing problem in American children and one that carries serious metabolic and cardiopulmonary consequences, including an increased risk of sleep-disordered breathing. Between 2009 and 2010, the prevalence of obesity in US children and adolescents was 16.9 %. [1] Worldwide, overweight and obesity estimates are approximately 43 million people; numbers continue to rise at alarming rates. [2]
Obesity in children is defined as body mass index (BMI) greater than or equal to the 95th percentile of the BMI for age as shown on growth charts of boys and girls aged 2-19 years. BMI percentiles are calculated based on sex and age reference charts and are used in contrast to absolute BMI because the amount of body fat changes with age and differs in boys and girls.
The spectrum of sleep disordered breathing ranges from habitual snoring, to upper airway resistance syndrome, to obstructive sleep apnea, and to obstructive apnea/hypoventilation syndrome. The presence of sleep-disordered breathing is an additional risk factor for cardiovascular morbidity in obese individuals and has been independently linked to metabolic syndrome. [2, 3] The behavioral and cognitive sequelae of sleep-disordered breathing both in children and adults have now been well described [4, 5, 6, 7] and have been listed in Clinical Presentation.
Obesity-hypoventilation syndrome (OHS), previously referred to as the Pickwickian syndrome, [8] is characterized by obesity, sleep-disordered breathing and chronic daytime alveolar hypoventilation (defined as Pa CO2 ≥45 mm Hg and Pa O2< 70). [9] The majority of patients with OHS have obstructive sleep apnea (90%); the remaining 10%, have sleep-hypoventilation. [10] Up to 20% of obese children have OHS. [11]
Education about pediatric sleep disorders is limited in US medical schools. Attempts are under way to improve awareness of sleep disorders and their impact on the health of children with obesity.
For patient education resources, see the Sleep Disorders Center.
Go to Obesity and Obesity in Children for complete information on this topic.
Pathophysiology and Etiology
Not all obese children develop obesity-hypoventilation syndrome (OHS). Causal factors leading to OHS are not completely understood. Most likely, complex interactions between obesity-related mechanical factors affecting lung function, altered respiratory drive, and sleep-disordered breathing contribute to the pathophysiology of OHS. [12]
Deficiency in leptin, a key hormone in appetite control and metabolism, has been implicated in ventilatory control, [13] pharyngeal collapsibility, [14] and upper airway function. [15]
Risk factors include the following:
-
Craniofacial abnormalities
-
Genetic syndromes (eg, Prader-Willi syndrome)
-
Central fat distribution
-
Severe obesity
Clinical Presentation
History
Daytime symptoms may include the following:
-
Audible mouth breathing
-
Daytime sleepiness
-
Hyperactivity
-
Morning headaches
-
Poor school performance and mathematical ability
-
Poor focus and visual-spacial skills
-
Poor memory and analytical thinking
-
Dyspnea
Sleep-related symptoms may include the following:
-
Habitual snoring
-
Restless sleep
-
Nocturnal enuresis
-
Witnessed apnea
-
Sleeping with head extended
Sleep apnea and daytime sleepiness can be aggravated by the use of alcohol, sedating antihistamines, CNS depressants, and some over-the-counter cold preparations.
Physical examination
General appearance
The assessment begins in the waiting room. Evaluate sleepy children who are consistently found sleeping in the waiting room or who cannot stay awake during the course of a physical examination.
Less than 10% of children who are obese have endogenous obesity. Therefore, each child should be assessed for dysmorphic features, short stature, and developmental delay.
Vital signs and work of breathing
Tidal volume is often decreased in obese children. They may increase their respiratory rate in order to increase their minute ventilation. Alternatively, they may hypoventilate.
Screen for hypertension. Hypertension in children is defined as systolic blood pressure, diastolic blood pressure, or both in the 95th percentile or higher on 3 or more separate visits.
Degree of obesity and fat distribution
Adjusted body mass index (BMI) in the 95th percentile or higher for age and sex is the most frequently used criterion to classify. BMI is inexpensive and easy to perform. It is calculated as weight (in kilograms) divided by height (in meters) squared.
Examination of the head and neck
Look for evidence of craniofacial dysmorphologies or anatomic obstruction that can impede upper airway volume. Examples include macroglossia; retrognathia or micrognathia; or oropharyngeal crowding secondary to enlarged tonsils, high-arched palate, dental malocclusions, large uvula, or low hanging soft palate.
Neck circumference is likely to be enlarged. Airway compression can be caused by excessive fatty tissue, thyroid enlargement, lymphadenopathy, cysts, or tumors.
Examination of the chest
Deformities of the chest wall such as thoracic kyphosis have been reported with extreme obesity. Acquired pectus excavatum has been described in children with obstructive sleep apnea syndrome. Some of the syndromes associated with sleep-disordered breathing, daytime somnolence, and obesity (eg, Prader-Willi syndrome) also are associated with an increased incidence of scoliosis.
Regarding lung examination, shallow respirations and evidence of dyspnea, especially with exertion, may occur in obesity-hypoventilation syndrome (OHS). Additional findings may suggest a primary pulmonary diagnosis.
Cor pulmonale is suggested by a displaced cardiac impulse and loud pulmonic second heart sound.
Fat distribution concentrated over the abdomen is associated with upward displacement of the diaphragm. The effects on respiration are more pronounced in the supine position.
Extremities
Ankle edema in this context is suggestive of congestive heart failure. Digital clubbing can been seen in children with congenital heart disease or chronic pulmonary conditions associated with hypoxia; it also may be familial.
Differential Diagnosis
Consider the following in the differential diagnosis:
-
Obstructive sleep apnea syndrome
-
Central hypoventilation syndromes
-
Narcolepsy
-
Sleep deprivation
-
Abuse of sedatives or antihistamines
-
Severe hypothyroidism
Diagnostic Testing
The diagnosis of obesity-hypoventilation syndrome (OHS) requires evidence of Pa CO2 greater than or equal to 45 mg Hg, evidence of sleep-disordered breathing, and obesity. Other causes of hypoventilation, including pulmonary disease, neuromuscular disease, chest wall disease, and other central control abnormalities, must be excluded. [18]
Screening tests
The tests most commonly used for screening include the following [18] :
-
Serum bicarbonate levels - A value of 27 mEq/L or greater (sensitive but not specific)
-
Pulse oximetry during wakefulness – Demonstrating low oxygen saturation on room air
-
Arterial blood gas measurements - Definite demonstration of elevated carbon dioxide and decreased oxygen levels
-
Attended laboratory nocturnal polysomnography - Criterion standard method for assessing sleep-disordered breathing in children; used to identify the presence and define the type and severity of sleep-disordered breathing; practice parameters and technical criteria used in children are summarized bu Aurora et al [19] and Marcus et al [20]
See the image below.
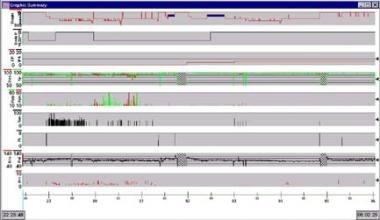 Histogram of overnight polysomnogram from patient with obesity and obstructive sleep apnea.
Histogram of overnight polysomnogram from patient with obesity and obstructive sleep apnea.
Other tests to consider
Supportive tests, tests of exclusion, and tests to evaluate for cor pulmonale are as follows:
-
Hematocrit level - To confirm the presence of polycythemia
-
Thyroid function studies - To evaluate the child for evidence of severe hypothyroidism
Learning, memory, and behavioral issues require specialized testing.
Imaging studies are as follows:
-
Lateral neck radiographs – Airway narrowing has been associated with higher diagnostic yields on nocturnal polysomnography [20]
-
Cephalometry - Can be used to demonstrate an association between a small mandible and obstructive sleep apnea
-
Chest radiographs (2 views) - Assist in the evaluation of chest wall deformity and cardiopulmonary abnormalities
Echocardiography and electrocardiography are as follows:
-
Complement the chest radiograph in the evaluation of the heart
-
Right ventricular hypertrophy/cor pulmonale, dysrhythmias, and right bundle-branch block have been reported in OHS
Pulmonary function testing in children with obesity
With flow volume loops, a sawtooth pattern associated with upper airway obstruction may be observed.
Spirometry is as follows:
-
Over 50% of obese children have abnormal pulmonary function findings, most of which are mild in nature [23]
-
Sex differences have been reported in the lung function of obese children
-
Forced vital capacity was significantly impacted in overweight boys but was not observed in girls who were overweight
-
Fat distribution in both overweight and obese adolescents differs from that seen in adults and is sex specific; boys tend to accumulate fat in the abdominal area, whereas girls tend to accumulate fat in the subscapular area [24]
Lung volume findings are as follows:
-
The expiratory reserve volume (ERV) is decreased, and, as a result, the forced vital capacity is also decreased
-
Bering et al [25] found ERV to be the most sensitive indicator of obesity
Diffusion testing results are as follows:
-
Studies of diffusion have yielded varying results
With body plethysmography testing, airway resistance is increased.
Tests to evaluate daytime sleepiness
The multiple sleep latency test [27] is indicated in the evaluation of individuals reporting hypersomnolence in order to objectively document sleepiness. It is performed on the day following the overnight polysomnogram. A mean sleep latency value of less than 5 or 6 minutes is indicative of pathologic sleepiness.
The Epworth Sleepiness Scale for Children [28, 29] is a modification based on the Epworth sleepiness scale. It is a self-administered questionnaire that asks the adolescent to use a 4 point scale (0-3) to rate their chance of dozing off or falling asleep in 8 different situations. Scores provide a general measure of sleepiness.
Treatment & Management
Surgical options
Adenotonsillectomy
This is considered the first-line treatment for children with obstructive sleep apnea. [30]
Perioperative risks [31, 32] are increased in individuals with obesity and sleep-disordered breathing. In addition to the risks of respiratory complications related to adenotonsillectomy performed for relief of upper airway obstruction, obese children with obstructive sleep apnea may experience complications related to the use of opiates in the postoperative period. [33]
Persistent findings of obstructive sleep apnea have been reported in some obese children following adenotonsillectomy. [34, 35] Postoperative polysomnograms should be considered in these children.
Weight-loss strategies should be implemented in conjunction with upper airway surgery. [36]
Bariatric surgery
Experience with bariatric surgery in children is limited, and the age at which it should be considered is controversial. [37, 38]
A recent review by Barnett discusses the various procedures—Roux en Y gastric bypass, adjustable gastric banding, and sleeve gastrectomy—noting a trend toward the use of sleeve gastrectomy in the adolescent patient population. [39] The data presented by Alqahtani et al on their experience with sleeve gastrectomy in severely obese children and adolescents aged 5-21 years showed a low complication rate, [40] with safety and efficacy profiles similar to that of adults. [41]
Best practice guidelines are available and consider physical maturity, ability to understand, degree of obesity, and comorbid conditions, including sleep apnea. [42]
Weight loss and weight maintenance therapy
In a comparison of weight management interventions for obese children involving diet versus diet plus exercise, diet plus exercise was associated with greater reductions in the metabolic risks. [43]
Positive pressure therapy
This is a noninvasive treatment option available in 2 modalities: continuous positive airway pressure (CPAP) and bilevel positive airway pressure (BiPAP). [44] This is considered first-line treatment in adults with obesity-hypoventilation syndrome (OHS) [45] but not in children. CPAP has been used safely in children and may be considered either when adenotonsillectomy is not an option or if it was not successful. [30]
Although positive pressure therapy in children has been shown to improve polysomnographic findings of obstructive sleep apnea and improve daytime sleepiness, adherence to therapy is often problematic. [46]
Pharmacologic therapy
The use of respiratory stimulants has been reported in the literature. However, their use is limited to small numbers or case reports.
Consultations
During the course of the evaluation, diagnosis, and treatment, pediatric healthcare teams may require consultation from members of the following subspecialties:
-
Pediatric sleep medicine
-
Pediatric endocrinology
-
Pediatric otolaryngology
-
Pediatric gastroenterology and nutrition
-
Genetics
-
Pediatric neurology
-
Pediatric intensive care
-
Bariatric surgeon
Long-term management
Patients being treated with noninvasive positive airway pressure should be monitored for the following:
-
Compliance
-
Progression of symptoms
-
Need for change in mask size or degree of support
-
Complications/adverse effects of treatment
-
Life-style changes and weight management
Further inpatient care
Obesity has strong links to metabolic syndrome, diabetes, and hypertension, which may complicate the treatment course.
Prevention
There is an increased incidence of obesity in adults who were obese as children or adolescents. Lifestyles that include exercise and good nutrition help to maintain good cardiovascular fitness and a healthy weight. Effective school-based interventions include support for an active lifestyle, nutritionally appropriate food options at school, and education about healthy decision making around food choices. [47]
Prognosis
Untreated obesity-hypoventilation syndrome (OHS) is associated with increased risk for respiratory, metabolic, hormonal, and cardiac impairment. Studies of adult patients have shown decreased quality of life, with higher rates of unemployment and poor social function. Healthcare costs are increased, as are the risks for hospitalization and early death. [48, 49]
-
Histogram of overnight polysomnogram from patient with obesity and obstructive sleep apnea.






