Practice Essentials
Epistaxis, or bleeding from the nose, is a common complaint. [1] It is rarely life threatening but may cause significant concern, especially among parents of small children. [2] Most nosebleeds are benign, self-limiting, and spontaneous, but some can be recurrent. Many uncommon causes are also noted. [3]
Epistaxis can be divided into 2 categories, anterior bleeds and posterior bleeds, on the basis of the site where the bleeding originates (see the image below).
The true prevalence of epistaxis is not known, because most episodes are self-limited and thus are not reported. When medical attention is needed, it is usually because of either the recurrent or severe nature of the problem. Treatment depends on the clinical picture, the experience of the treating physician, and the availability of ancillary services. [4, 5, 6, 7]
Workup in epistaxis
If a history of persistent heavy bleeding is present, obtain a hematocrit count and type and cross match. If a history of recurrent epistaxis, a platelet disorder, or neoplasia is present, obtain a complete blood count (CBC) with differential. The bleeding time is an excellent screening test if suspicion of a bleeding disorder is present. Obtain the international normalized ratio (INR)/prothrombin time (PT) if the patient is taking warfarin or if liver disease is suspected. Obtain the activated partial thromboplastin time (aPTT) as necessary.
With regard to visual evaluation, direct visualization with a good directed light source, a nasal speculum, and nasal suction should be sufficient in most patients. However, computed tomography (CT) scanning, magnetic resonance imaging (MRI), or both may be indicated to evaluate the surgical anatomy and to determine the presence and extent of rhinosinusitis, foreign bodies, and neoplasms. Nasopharyngoscopy may also be performed if a tumor is the suspected cause of bleeding.
Management of epistaxis
In most patients with epistaxis, the bleeding responds to cauterization, nasal packing, or both. For those who have recurrent or severe bleeding for which medical therapy has failed, various surgical options are available. After surgery or embolization, patients should be closely observed for any complications or signs of rebleeding.
Medical approaches to the treatment of epistaxis may include the following:
-
Adequate pain control in patients with nasal packing, especially in those with posterior packing (However, the need of adequate pain control has to be balanced with the concern over hypoventilation in the patient with posterior pack.)
-
Oral and topical antibiotics to prevent rhinosinusitis and possibly toxic shock syndrome
-
Avoidance of aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs)
-
Medications to control underlying medical problems (eg, hypertension, vitamin K deficiency) in consultation with other specialists
Arterial ligation
The choice of the specific vessel or vessels to be ligated depends on the location of the epistaxis. In general, the closer the ligation is to the bleeding site, the more effective the procedure tends to be. Ligation of the external carotid artery (ECA) can be performed with the patient under local or general anesthesia. Internal maxillary artery ligation has a higher success rate than ECA ligation because of the more distal site of intervention.
If bleeding occurs high in the nasal vault, consider ligation of the anterior ethmoidal artery, the posterior ethmoidal artery, or both. These arteries are approached through an external ethmoidectomy incision.
Embolization
Bleeding from the ECA system may be controlled with embolization, either as a primary modality in poor surgical candidates or as a second-line treatment in those for whom surgery has failed.
Also see Anterior Epistaxis Nasal Pack, Posterior Epistaxis Nasal Pack, and Surgery for Pediatric Epistaxis.
Anatomy
The nose has a rich vascular supply, with substantial contributions from the internal carotid artery (ICA) and the external carotid artery (ECA).
The ECA system supplies blood to the nose via the facial and internal maxillary arteries. The superior labial artery is one of the terminal branches of the facial artery. This artery subsequently contributes to the blood supply of the anterior nasal floor and anterior septum through a septal branch.
The internal maxillary artery enters the pterygomaxillary fossa and divides into 6 branches: posterior superior alveolar, descending palatine, infraorbital, sphenopalatine, pterygoid canal, and pharyngeal.
The descending palatine artery descends through the greater palatine canal and supplies the lateral nasal wall. It then returns to the nose via a branch in the incisive foramen to provide blood to the anterior septum. The sphenopalatine artery enters the nose near the posterior attachment of the middle turbinate to supply the lateral nasal wall. It also gives off a branch to provide blood supply to the septum.
The ICA contributes to nasal vascularity through the ophthalmic artery. This artery enters the bony orbit via the superior orbital fissure and divides into several branches. The posterior ethmoidal artery exits the orbit through the posterior ethmoidal foramen, located 2-9 mm anterior to the optic canal. The larger anterior ethmoidal artery leaves the orbit through the anterior ethmoidal foramen (see the image below).
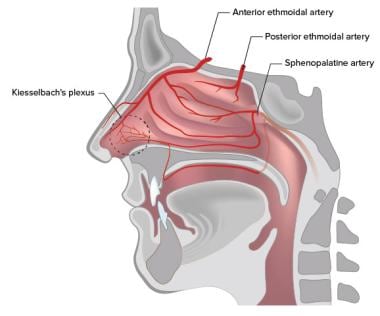
The anterior and posterior ethmoidal arteries cross the ethmoidal roof to enter the anterior cranial fossa and then descend into the nasal cavity through the cribriform plate. Here, they divide into lateral and septal branches to supply the lateral nasal wall and the septum.
The Kiesselbach plexus, or Little’s area, is an anastomotic network of vessels located on the anterior cartilaginous septum. It receives blood supply from both the ICA and the ECA. [8] Many of the arteries supplying the septum have anastomotic connections at this site.
Pathophysiology
Bleeding typically occurs when the mucosa is eroded and vessels become exposed and subsequently break.
More than 90% of bleeds occur anteriorly and arise from Little’s area, where the Kiesselbach plexus forms on the septum. [9, 10] The Kiesselbach plexus is where vessels from both the ICA (anterior and posterior ethmoidal arteries) and the ECA (sphenopalatine and branches of the internal maxillary arteries) converge. These capillary or venous bleeds provide a constant ooze, rather than the profuse pumping of blood observed from an arterial origin. Anterior bleeding may also originate anterior to the inferior turbinate.
Posterior bleeds arise further back in the nasal cavity, are usually more profuse, and are often of arterial origin (eg, from branches of the sphenopalatine artery in the posterior nasal cavity or nasopharynx). A posterior source presents a greater risk of airway compromise, aspiration of blood, and greater difficulty controlling bleeding.
Etiology
Causes of epistaxis can be divided into local causes (eg, trauma, mucosal irritation, septal abnormality, inflammatory diseases, tumors), systemic causes (eg, blood dyscrasias, arteriosclerosis, hereditary hemorrhagic telangiectasia), and idiopathic causes. Local trauma is the most common cause, followed by facial trauma, foreign bodies, nasal or sinus infections, and prolonged inhalation of dry air. Children usually present with epistaxis due to local irritation or recent upper respiratory infection (URI).
In a retrospective cohort study of 2405 patients with epistaxis (3666 total episodes), Purkey et al used multivariate analysis to identify a series of risk factors for nosebleeds. The likelihood of epistaxis was found to increase in patients with allergic rhinitis, chronic sinusitis, hypertension, hematologic malignancy, coagulopathy, or, as mentioned, hereditary hemorrhagic telangiectasia. The investigators also found increased nosebleeds in association with older age and colder weather. [11]
Similarly, a German study, by Seidel et al, found that the rate of patients receiving a first epistaxis diagnosis at an otolaryngologic practice was lowest in summer, with the rate increasing in fall and winter and peaking in February, March, and April. The study, which involved 114 otolaryngologic practices, reported a rate of 7.22 epistaxis patients per practice in August 2016, the lowest figure that year, compared with a peak rate of 14.89 patients per practice, in February 2016. [12]
Trauma
Self-induced trauma from repeated nasal picking can cause anterior septal mucosal ulceration and bleeding. This scenario is frequently observed in young children. Nasal foreign bodies that cause local trauma (eg, nasogastric and nasotracheal tubes) can be responsible for rare cases of epistaxis.
Acute facial and nasal trauma commonly leads to epistaxis. If the bleeding is from minor mucosal laceration, it is usually limited. However, extensive facial trauma can result in severe bleeding requiring nasal packing. In these patients, delayed epistaxis may signal the presence of a traumatic aneurysm.
Patients undergoing nasal surgery should be warned of the potential for epistaxis. As with nasal trauma, bleeding can range from minor (due to mucosal laceration) to severe (due to transection of a major vessel).
Dry weather
Low humidity may lead to mucosal irritation. Epistaxis is more prevalent in dry climates and during cold weather due to the dehumidification of the nasal mucosa by home heating systems.
Drugs
Topical nasal drugs such as antihistamines and corticosteroids may cause mucosal irritation. Especially when applied directly to the nasal septum instead of the lateral walls, they may cause mild epistaxis. Medications such as nonsteroidal anti-inflammatory drugs (NSAIDs) are also frequently involved.
Septal abnormality
Septal deviations (deviated nasal septum) and spurs may disrupt the normal nasal airflow, leading to dryness and epistaxis. The bleeding sites are usually located anterior to the spurs in most patients. The edges of septal perforations frequently harbor crusting and are common sources of epistaxis.
Inflammation
Bacterial, viral, and allergic rhinosinusitis causes mucosal inflammation and may lead to epistaxis. Bleeding in these cases is usually minor and frequently manifests as blood-streaked nasal discharge.
Granulomatosis diseases such as sarcoidosis, Wegener granulomatosis, tuberculosis, syphilis, and rhinoscleroma often lead to crusting and friable mucosa and may be a cause of recurrent epistaxis.
Young infants with gastroesophageal reflux into the nose may have epistaxis secondary to inflammation.
Tumors
Benign and malignant tumors can manifest as epistaxis. Affected patients may also present with signs and symptoms of nasal obstruction and rhinosinusitis, often unilateral.
Intranasal rhabdomyosarcoma, although rare, often begins in the nasal, orbital, or sinus area in children. Juvenile nasal angiofibroma in adolescent males may cause severe nasal bleeding as the initial symptom.
Blood dyscrasias
Congenital coagulopathies should be suspected in individuals with a positive family history, easy bruising, or prolonged bleeding from minor trauma or surgery. Examples of congenital bleeding disorders include hemophilia and von Willebrand disease. [8]
Acquired coagulopathies can be primary (due to the diseases) or secondary (due to their treatments). Among the more common acquired coagulopathies are thrombocytopenia and liver disease with its consequential reduction in coagulation factors. Even in the absence of liver disease, alcoholism has also been associated with coagulopathy and epistaxis. Oral anticoagulants predispose to epistaxis.
Vascular abnormalities
Arteriosclerotic vascular disease is considered a reason for the higher prevalence of epistaxis in elderly individuals.
Hereditary hemorrhagic telangiectasia (HHT; also known as Osler-Weber-Rendu syndrome) is an autosomal dominant disease associated with recurrent bleeding from vascular anomalies. The condition can affect vessels ranging from capillaries to arteries, leading to the formation of telangiectasias and arteriovenous malformations. Pathologic examination of these lesions reveals a lack of elastic or muscular tissue in the vessel wall. As a result, bleeding can occur easily from minor trauma and tends not to stop spontaneously.
Various organ systems such as the respiratory, gastrointestinal, and genitourinary systems may be involved. The epistaxis in these individuals is variable in severity but is almost universally recurrent.
Other vascular abnormalities that predispose to epistaxis include vascular neoplasms, aneurysms, and endometriosis.
Migraine
Children with migraine headaches have a higher incidence of recurrent epistaxis than children without the disease. [13] The Kiesselbach plexus, which is part of the trigeminovascular system, has been implicated in the pathogenesis of migraine. [14]
Hypertension
The relationship between hypertension and epistaxis is often misunderstood. Patients with epistaxis commonly present with an elevated blood pressure. Epistaxis is more common in hypertensive patients, perhaps owing to vascular fragility from long-standing disease.
Hypertension, however, is rarely a direct cause of epistaxis. More commonly, epistaxis and the associated anxiety cause an acute elevation of blood pressure. Therapy, therefore, should be focused on controlling hemorrhage and reducing anxiety as primary means of blood pressure reduction.
A study by Sarhan and Algamal, which included 40 patients with epistaxis and 40 controls, reported that the number of attacks of epistaxis was higher in patients with a history of hypertension, but the investigators were unable to determine whether a definite link existed between nosebleeds and high blood pressure. They did find, however, that control of epistaxis was more difficult in hypertensive patients; patients whose systolic blood pressure was higher at presentation tended to need management with packing, balloon devices, or cauterization. [15]
Excessive coughing causing nasal venous hypertension may be observed in pertussis or cystic fibrosis.
Idiopathic causes
The cause of epistaxis is not always readily identifiable. Approximately 10% of patients with epistaxis have no identifiable causes even after a thorough evaluation. [16]
Epidemiology
The frequency of epistaxis is difficult to determine because most episodes resolve with self-treatment and, therefore, are not reported. [17] However, when multiple sources are reviewed, the lifelong incidence of epistaxis in the general population is about 60%, with fewer than 10% seeking medical attention. [8, 18, 17]
The age distribution is bimodal, with peaks in young children (2-10 y) and older individuals (50-80 y). Epistaxis is unusual in infants in the absence of a coagulopathy or nasal pathology (eg, choanal atresia, neoplasm). Local trauma (eg, nose picking) does not occur until later in the toddler years. Older children and adolescents also have a less frequent incidence. Consider cocaine abuse in adolescent patients.
Prevalence of epistaxis tends to be higher in males (58%) than in females (42%).
Prognosis
For most of the general population, epistaxis is merely a nuisance. However, the problem can occasionally be life-threatening, especially in elderly patients and in those patients with underlying medical problems. Fortunately, mortality is rare and is usually due to complications from hypovolemia, with severe hemorrhage or underlying disease states.
Overall, the prognosis is good but variable; with proper treatment, it is excellent. When adequate supportive care is provided and underlying medical problems are controlled, most patients are unlikely to experience any rebleeding. Others may have minor recurrences that resolve spontaneously or with minimal self-treatment. A small percentage of patients may require repacking or more aggressive treatments.
Patients with epistaxis that occurs from dry membranes or minor trauma do well, with no long-term effects. Patients with HHT tend to have multiple recurrences regardless of the treatment modality. Patients with bleeding from a hematologic problem or cancer have a variable prognosis. Patients who have undergone nasal packing are subject to increased morbidity. Posterior packing can potentially cause airway compromise and respiratory depression. Packing in any location may lead to infection.
Patient Education
For patient education resources, see the Breaks, Fractures, and Dislocations Center, as well as Broken Nose.
The following precautions should be imparted to the patient:
-
Use nasal saline spray.
-
Avoid hard nose blowing or sneezing.
-
Sneeze with the mouth open.
-
Do not use nasal digital manipulation.
-
Avoid hot and spicy foods.
-
Avoid taking hot showers.
-
Avoid aspirin and other NSAIDs.
The following simple instructions for self-treatment for minor epistaxis should be provided:
-
Apply firm digital pressure for 5-10 minutes.
-
Use an ice pack.
-
Practice deep, relaxed breathing.
-
Use a topical vasoconstrictor.
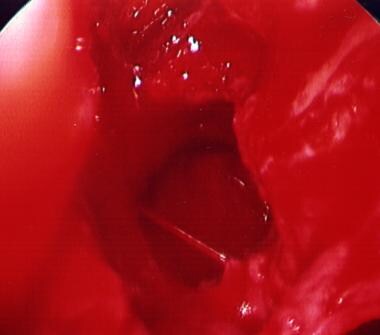
-
Posterior epistaxis from the left sphenopalatine artery.
-
Resolved posterior epistaxis after endoscopic cauterization of the left sphenopalatine artery.
-
Nasal speculum.
-
Vaseline gauze packing.
-
Expandable (Merocel) packing (dry).
-
Nasal vascular anatomy
Tables

What would you like to print?
- Overview
- Presentation
- DDx
- Workup
- Treatment
- Approach Considerations
- Manual Hemostasis
- Humidification and Moisturization
- Cauterization
- Nasal Packing
- Arterial Ligation
- Embolization
- Palliative Therapy for Hereditary Hemorrhagic Telangiectasia
- Complications of Treatment
- Dietary Measures
- Activity Restriction
- Prevention of Epistaxis
- Consultations
- Long-Term Monitoring
- Show All
- Guidelines
- Medication
- Questions & Answers
- Media Gallery
- References




