Background
People are exposed to aeroallergens in various settings, both at home and at work. Fungi are ubiquitous airborne allergens and are important causes of human diseases, especially in the upper and lower respiratory tracts. These diseases can occur in persons of various ages.
Exposure to molds can cause human disease through several well-defined mechanisms. In addition, many new mold-related illnesses have been hypothesized in recent years that remain largely or completely unproven. Concern about mold exposure and its effects are so common that all health care providers are frequently faced with issues regarding these real and asserted mold-related illnesses.
Fungi as aeroallergens
Airborne spores and other fungi particles are ubiquitous in nonpolar landscapes, especially among field crops, and often form the bulk of suspended biogenic debris. The term mold is often used synonymously with the term fungi. A definition more precise than this specifies that molds lack macroscopic reproductive structures but may produce visible colonies. Respiratory illness in subjects exposed to rust and dark-spored imperfect fungi was described more than 60 years ago, and human sensitization to diverse fungi is now well recognized. Because fungus particles are commonly derived from wholly microscopic sources, exposure hazards are assessed by directly sampling a suspect atmosphere in most circumstances. Because of their small size, fungal emanations present special collection requirements to ensure particle viability for culture-based studies.
Functional biology of fungi
Fungi have 2 basic structures. Yeast grows as single cells by means of central division of eccentric buds to form daughter units. Most other familiar fungi are composed of branching threads, 3-10 µm in width, termed hyphae. A mycelium is an aggregate of hyphae. Hyphae are modified to bear the simple reproductive parts of many microfungi and form the structural tissue of fleshy fungi (eg, mushrooms, puff balls).
In general, familiar allergenic molds reproduce asexually. However, 2 large and distinctive classes, Ascomycetes and Basidiomycetes, also produce innumerable sexual spores for atmospheric dispersion. In its life cycle, a single fungus organism produces both sexual and asexual spores from morphologically different structures respectively termed perfect and imperfect stages.
In considering known and potential allergens, 5 major classes of fungi have particular clinical significance: Oomycetes, Zygomycetes, Ascomycetes, Basidiomycetes, and Deuteromycetes.
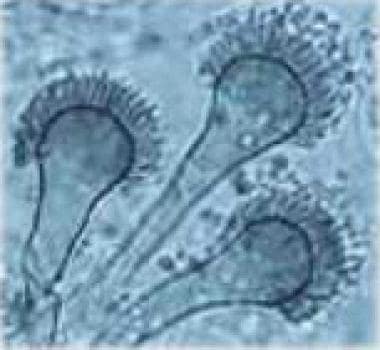
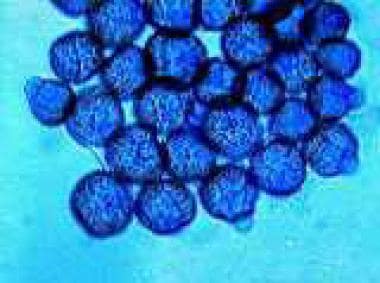
Most molds require elemental oxygen during growth. Traces of formed carbohydrate are also essential. Vegetative hyphae of most fungi grow best at 18-32°C, and, although most become dormant at subfreezing temperatures, a few may sporulate below 0°C. At the other extreme, although 71°C is generally lethal for molds, certain types thrive at slightly cooler temperatures. Aspergillus fumigatus and Aspergillus niger tolerate a wide range of temperatures (see the image below).
Atmospheric moisture affects not only the growth and fruiting of fungi but also the dispersion of spores and resultant prevalence. Spore counts typically rise with rainfall and fog and with damp, nocturnal conditions. Rain and dew splash also foster dispersion of slime spores. As a result, atmospheric recoveries of Fusarium, Phoma, Cephalosporium, and Trichoderma species peak with rainfall.
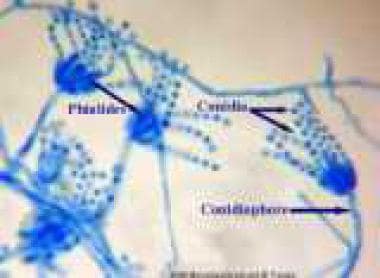
The reproductive units of many fungi are detached by direct wind scouring or wind-induced substrate motion. Such dry spore dispersal increases as airspeed rises and relative humidity falls, peaking often during summer afternoons. At such time, typical spores of Cladosporium, Alternaria, Epicoccum, Helminthosporium, Rhizopus, Aspergillus, and Penicillium species may also peak (see the images below).




The circadian trends in changes of temperature, humidity, airspeed, and light intensity frequently interact to promote diurnal airborne spore levels. All data emphasize that regional vegetation strongly affects the local airborne spore levels.
Assessing the prevalence of fungi in air
Studies of airborne fungi provide prevalence data that are important to estimate patients' exposures to molds. A common method of sampling molds is to use an Anderson air-sample volumetric collector (Anderson Instruments; Atlanta, Georgia). The collector machine is allowed to sample the designated space for 5 minutes, trapping air particles in the filter. The filter then is placed on a Petri dish with media containing Sabouraud glucose, potato dextrose, and malt extract agar. Colonies grow on the agar plate, which an experienced mycologist can often use to identify the species on the basis of its gross appearance. Spore counts may be expressed as the number of colonies from a cubic meter of air. If the counts are higher than 200 spores in a cubic meter of air, patients with allergy are most likely to have symptoms.
Clinical relevance of allergenic fungi
Several fungal species (usually molds) cause allergic reactions in humans. The most common and best described mold allergen sources belong to the taxonomic group fungi imperfecti (usually asexual stages of Ascomycetes), which includes Alternaria, Cephalosporium, and Aspergillus species. Species of Basidiomycetes and yeast, such as Candidiasis albicans, are also important allergen sources.
Alternaria and Cladosporium species are common in outdoor environments worldwide. Airborne spores and mycelium debris of Cladosporium and Alternaria species are present during spring, summer, and especially autumn because of the degradation of leaves and other biomaterial. In indoor environments, Aspergillus and Penicillium species predominate with relatively few characteristic seasonal changes.
In early 1970, the United States faced an unexpected energy crisis because of the political climate in the world. The heavy dependence on foreign oil suddenly became a national issue. In responding to the call for conservation, the housing industry used more energy-saving insulation in buildings. However, the heavy insulation unexpectedly resulted in an excessive increase of humidity inside those buildings. This led to increase in mold-related health issues because the increased humidity led to higher mold counts within the buildings.
Similarities of allergen epitopes (antigenic [Ag] determinants) have been reported among some mold species, as observed in the closely related genera Alternaria and Stemphyllium. Otherwise, no immunochemical similarities have been detected among the major allergens of these species. The preparation of allergen extracts from cultured mold is very difficult secondary to low protein and high carbohydrate contents and the presence of potent proteolytic enzymes.
The Pollution and the Young (PATY) study included more than 58,000 children. [1] The study was conducted in Russia, North America, and 10 countries in Western Europe. The children were aged 6-12 years. The investigators studied the association between visible molds reported in the household and a spectrum of 8 respiratory and allergic symptoms within each study. Positive association between exposure to mold and children's respiratory symptoms were consistently noted across studies and across outcomes. For instance odds ratios ranged from 1.3 (95% confidence interval [CI], 1.22-1.39) for nocturnal cough to 1.5 (95% CI, 1.31-1.73) for morning cough.
A study in Finland showed the most common mold to induce occupational rhinitis was A fumigatus. [2] Association between the immunoglobulin E (IgE) sensitization and exposure level was statistically significant. The mold that grew in conjunction with moisture damage was the leading cause of occupational rhinitis.
A study indicated that IgE sensitization of fungi mirrors fungal phylogenetic systematics. [3] A database was compiled from recorded serum IgE antibody levels in response to 17 different fungal species from 668 individuals sensitized to at least one of the 17 species. By applying a cluster method to this data set, the fungal species were grouped into a hierarchical organization. The resulting organization was compared with published fungi findings. The results of this study showed that the hierarchical structure of fungi based in IgE antibodies in sensitized individuals reflected the phylogenetic relationship. Examples include the distinct separation of basal fungi from the subkingdom Dikarya, as well as individual cluster formations of fungi belonging to the subphylum Saccharomycotina and order Pleosporales.
This is the first study that demonstrates a close relationship between molecular fungal systematics and IgE sensitization to fungal species. Because close evolutionary organisms typically have a higher degree of protein similarity, IgE cross reactivity is likely the main reason for obtained organization.
Culturable molds in indoor air and the association with moisture-related problems and asthma and allergy among Swedish children has been reported. [3] Although mold spore exposure indoors has been suggested as a possible explanation for airway problems such as asthma and allergy among people living in buildings with moisture-related problems, this study could not find any associations between the spore concentrations in indoor air and signs of dampness and moldy odor reported by parents or observed by professional inspectors.
No association between the indoor spore concentration and asthma or allergy among children was noted. With these results, the authors concluded that one-time air sampling of mold colony-forming unit (CFU) in indoor air was not indicated to identify risk factors for asthma or allergy in children living in Scandinavian countries.
In contrast, in a study of environmental factors associated with poor asthma control in Montreal, suboptimal asthma appeared to be mostly associated with traffic, along with mold and moisture conditions. [4] The mold and moisture control thus have a greater public health impact.
In another European study, authors reviewed the projection of the effects of climate change on allergic asthma, in particular the contribution of aerobiology. [5] The authors believe climate change is unequivocal and reprensts a possible threat for patients affected by allergic conditions. However, they acknowledged numerous limitations that make prediction uncertain. More stress on pollen and spore exposure in the diagnosis and treatment guidelines of respiratory and allergic diseases are recommended. Collection of aerobiological data in a structured way at the European level and support of multidisciplinary research teams in this area was highly emphasized.
In one study in the United Kingdom in the asthmatic patients, it was shown that Aspergillus fumigates detection in sputum is associated with A fumigates -IgE sensitization, neutrophilic airway inflammation, and reduced lung function compared to asthmatics with IgG sensitization or asthmatics without sensitization to A fumigatus. This supports the concept that allergic inflammation could significantly lead to fixed airway obstruction in asthma, as illustrated with effect of airway colonization and sensitivity with A fumigatus. [6]
One of the problems with mold exposure estimates is the lack of quantitative, standardized methods for describing the residential mold burden. A metric called the Environmental Relative Moldiness Index (ERMI) has been developed and validated in a national survey of homes. [7] A DNA-based, mold-specific quantitative polymerase chain reaction of 26 species formed the basis of the ERMI. The ERMI scale usually ranges from approximately -10 to 20 and is divided into quartiles, with the highest-quartile homes (ERMI value >5) having the highest mold burden. [7]
Pathophysiology
Immunologic evolution of allergy
Allergen-specific IgE produced by B cells mediate allergic diseases. The allergen sensitization begins with the processing of mold Ags by Ag-presenting cells (APC), such as dendritic cells. APCs present processed mold allergens to naive T-helper (Th) cells, which differentiate into the effector stage type 2 Th (Th2) cells and produce Th2 cytokines (interleukin [IL]-4, IL-5, and IL-13). IL-4 is essential for isotype switching to IgE and with additional signaling provided by the Th2 cells, B cells begin to produce IgE specific for allergens.
The Fc portion of IgE antibody binds to high-affinity Fcε receptors (FcεR) expressed on the cell surface of mast cells in tissue, which, in turn, stabilizes Fcε. IgE bound to FcεR is stable for several weeks. When allergens bind to adjacent 2 IgE molecules bound to FcεR (cross-linking), an activation signal is elicited, leading to the release of preformed and newly formed mediators from mast cells (mast-cell activation).
These mediators include histamine, leukotrienes, and prostaglandins, which cause acute tissue inflammation. Mast-cell activation also lead to release of various chemotactic factors, such as leukotriene B4, platelet-activating factor, and eosinophil chemotactic factor, resulting in an influx of eosinophils, neutrophils, and mononuclear cells into the site of mast-cell activation. Mast cells also produce IL-4, IL-5, and IL-13, further augmenting Th2 responses and IgE production.
Granulocyte-macrophage colony-stimulating factor (GM-CSF), IL-3, and IL-5 derived from Th2 cells, mast cells, and other lineage cells induce the differentiation of eosinophil precursors in the bone marrow. IL-5 is thought to be crucial for eosinophil trafficking to the peripheral circulation, leading to eosinophilia. Various chemotactic factors, including chemokines, then recruit eosinophils to the site of allergen exposure. Thus, IgE-mediated immune reactions result in eosinophil-dominant inflammation. The initial inflammatory process initiated by mold allergens may be further compounded by the waves of inflammatory cell infiltration. Clinical features of mold allergy differ in the upper or lower respiratory tract that can also vary in each individual, influenced by age, genetic predisposition, exposure to other environmental allergens-irritants, etc.
Th2 responses are predominant to immune responses to mold allergens, but a type 1 T-helper (Th1) response characterized by cell-mediated immunity may also contribute to mold-induced inflammatory condition. The known clinical disorders related to immune reactions to molds are listed below.
Mold-induced respiratory symptoms may be notably delayed at the onset, and they may be associated with bacterial superinfection. This may reflect the fact that the concomitant microbial agents (and endotoxin) present in wild sources of mold growth, such as dusts from decomposing plant material, can compound the clinical manifestations.
Determinants of allergic fungi
The cross-reactivity (shared epitopes) of allergens derived from common airborne fungus spores remains controversial. Allergenic cross-reactivity such as observed between Phoma and Alternaria extracts more likely reflect the presence of shared epitopes in the species' reproductive stages. Establishing biologic or allergenic properties among molds is difficult, especially imperfect fungi. Therefore, defining Ag determinants is important when a mold allergen extract is prepared.
Total airborne fungi in North America range from extremely low levels during periods of below-freezing temperature to peak levels that usually occur in late summer and early autumn. This pattern parallels variations in dominant Cladosporium and Alternaria species in many areas. Penicillium species most often lack a defined annual pattern; A fumigatus may be more prominent from December-April in some areas but can be unpredictable in other regions. Mold allergy may account for persistent respiratory symptoms in individuals during nonpollen seasons.
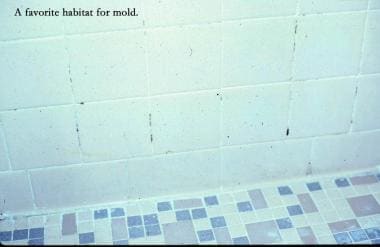
Fungi readily invade indoor environments, and indoor growth can cause perennial allergic symptoms. Penicillium and Aspergillus species are commonly found in enclosed spaces, followed by Rhizopus and Mucor species. Soiled upholstery and garbage containers are favored sites of indoor fungal growth. The porosity of rubber and synthetic foams and their tendency to remain moist favor fungalgrowth.Basements, window molding, shower curtains, and plumbing fixtures are common sites for indoor fungal growth (see the image below).
Poorly maintained cold-mist vaporizers and some console humidifiers can emit dense microbial aerosols during operation. If high relative humidity and condensation persist in indoor environments, mold is likely to recur after decontamination.
The clinical relevance of cross-reactivity among the different fungal species has been largely unknown. However, progress in molecular cloning of fungal allergens and the availability of more than 40 completely sequenced fungal genomes facilitates characterization, cloning, and production of highly pure recombinant allergens; identification of homologous and orthologous allergens; in silico prediction; and experimental in vitro and in vivo verification of cross-reactivity between homologous panallergens. [8] These studies indicate that cross-reactivity is an important component of fungal sensitization.
However, a new study among Swedish children indicated that no association was found between the spore concentration and signs of dampness and moldy odor reported by parents or by professional inspectors. No association was found between the indoor spore concentration and asthma or allergy among children. Thus, one-time air sampling of mold CFU in indoor air is not indicated to identify risk factors for asthma or allergy in children living in Scandinavian countries.
Contradictory to the above study, a population-based study in Montreal children suggests home environmental factors associated with poor asthma control. [4] Of 980 children with active asthma, 36% met criteria of poor control of their diseases. The population's characteristics were related with lack of asthma control, after adjustment, and included children living along high-traffic density streets (PR, 1.35; 95% CI, 1-1.81) and those with their bedroom or residence at the basement level (PR, 1.30; 95% CI, 1.01-1.66). The study concluded suboptimal asthma control appears to be associated with traffic, along with mold and moisture conditions; the latter is a more frequent exposure and, therefore, has a greater public health impact.
The therapeutic potential of pathogen-derived products
Several pathogen-derived products have been shown to possess therapeutic potentials for allergic diseases. It has been suggested the glucan of the wall component of a variety of fungi may have that potential. Kawashima et al, using an animal study, examined the effect of curdlan, a linear beta-(1-3)-glucan, on the development of allergic airway inflammation. [9] They found that an injection of curdlan significantly inhibited Ag-induced eosinophilic recruitment and Th2 cytokine productions in the airways. They found that STAT6-aided IL-10 production by CD4+ T cells in the presence of curdlan contributed to this process. It underscores the therapeutic potential of curdlan for various fungus-related allergic diseases.
Animal models of allergic airway diseases
Animal models of disease are an invaluable tool for contributing to the understanding of the pathophysiology of allergic airway diseases. Hoselton et al reported such model using A fumigatus. Balb/c mice were challenged with A fumigatus via intranasal inoculation. They were previously sensitized with intraperitoneal injections with soluble A fumigatus in alum. After a single challenge of inhalation, allergic pulmonary inflammation and airway hyperresponsiveness were significantly increased compared with control animals. Later, a significant increase in epithelial thickness, global cell metaplasia, and peribronchial collagen deposition was noted. The authors concluded this was the first time they demonstrated that the consistent development of fibrosis and smooth muscle changes accompany exposure to inhaled fungal conidia in a mouse model.
Clinical forms of mold allergy - Allergic rhinitis, allergic conjunctivitis and allergic asthma
Allergic rhinitis and/or allergic conjunctivitis are common problems in both children and adults. Allergic rhinitis or allergic conjunctivitis is usually a perennial problem, with seasonal fluctuation of symptoms in regions such as the southern part of the United States, where humidity and temperatures are high.
Many indoor fungal allergens (eg, Alternaria, Aspergillus, Cephalosporium, Curvularia, Epicoccum, Fusarium, Helminthosporium, Hormodendrum, Mucor, Penicillium, Phoma, Pullularia, Rhizopus, and Stemphylium species) can cause allergic symptoms. They are the result of type 1 (IgE-mediated) hypersensitivity reactions.
Patients should have detectable IgE antibody to provoke mast-cell activation with fungal exposure. Studies also indicated the close association of mold allergy with prolonged coldlike symptoms in winter, sinusitis, and the presence of adenoid hypertrophy in children. [10]
Allergic asthma or IgE-mediated asthma: Patients with fungal spore–induced asthma often have IgE antibodies to more prevalent fungi, such as Alternaria and Cephalosporium species. As many as 25% of patients with asthma have skin prick test reactivity to a mixture of 4 species of Aspergillus. The fungal allergen-induced asthma can occur in both children and adults as a result of a type 1 hypersensitivity reaction. These patients manifest potent late-phase reactions.
Clinical forms of mold allergy - Allergic fungal sinusitis (AFS)
Allergic Aspergillus sinusitis primarily occurs in patients with nasal polyps and mucoid impaction of the sinuses. The mucus typically contains eosinophils, Charcot-Leyden crystals (breakdown products of eosinophils), and hyphae of A fumigatus. AFS can also be induced with exposure to other fungi, including Bipolaris, Curvularia, Alternaria, Exserohilum, Helminthosporium, and Rhizopus species. This condition is relatively rare in the pediatric population and is a result of type 1, type 3 (immune complex), and type 4 (delayed type) hypersensitivity reactions. Manning et al reported on 6 patients aged 8-16 years who had findings typical to allergic Aspergillus sinusitis. [11]
A review of allergic fungal rhinitis and rhinosinusitis indicated epidemiologic studies have failed to demonstrate a direct relationship between fungal allergy and allergic rhinitis either via outdoor or indoor exposure. [5] The author indicated fungal allergy is clearly linked to a subset of chronic rhinosinusitis (CRS) known as allergic fungal rhinosinusitis (AFRS). The condition represents an intense allergic response against colonizing fungi that give rise to formation of allergic (eosinophilic) mucin, mucostasis, and sinus opacification.
A broader role for colonizing fungi has been postulated in CRS, owing to the demonstration of fungi in mucus in the vast majority of cases of CRS and in vitro studies that have demonstrated certain fungi, particularly Alternaria, modify an allergic response in patients with CRS that is independent of IgE.
Clinical forms of mold allergy - Allergic bronchopulmonary aspergillosis (ABPA)
This is a well-recognized form of hypersensitivity pneumonitis, with nearly every case occurring in patients with previously diagnosed asthma or cystic fibrosis (CF).
ABPA rarely occurs in the absence of clinical asthma. The pulmonary immune system responds to a saprophytic fungus present in bronchial mucus, leading to bronchial wall widening (bronchiectasis) and distal small-airway fibrosis (bronchiolitis obliterans). It is characterized by clinical, immunologic, radiologic, and pathologic findings that range from mild asthma to end-stage fibrotic lung disease.
Children with CF are susceptible to ABPA with mucoid impaction of Aspergillus species. A fumigatus is the most frequent Aspergillus species to infect humans. Spores are 2-3.5 µm, which permits penetration to smaller airways. ABPA is the result of types 1, 3, and 4 hypersensitivity reactions.
Clinical forms of mold allergy - Non-Aspergillus allergic bronchopulmonary mycosis (ABPM)
The most common cause of ABPM is C albicans. Isolated cases of ABPM caused by other fungi in asthma patients have been described; pathogens included Cladosporium and Curvularia species. ABPM has been described in patients with CF. A child with CF was reported to have developed ABPM with Trichosporon beigelii. [12] The disease is the result of types 1, 3, and 4 hypersensitivity reactions.
Clinical forms of mold allergy - Extrinsic allergic alveolitis (EAA)
EAA encompasses a broad spectrum of pulmonary interstitial and alveolar diseases caused by repeated (occupational) exposure to a wide variety of organic dusts, microbes, and chemicals.
Repeated exposure to various molds can also cause EAA. Mold-induced EAA includes wood pulp worker's lung (Alternaria species), malt worker's lung (Aspergillus clavatus), farmer's lung (A fumigatus), maple bark stripper's lung (Cryptostroma corticale), and sewage worker's lung (Cephalosporium species).
The inflammatory process of EAA involves mast-cell activation, immune complex formation (type 3 hypersensitivity tissue injury), and influx of immune cells producing proinflammatory cytokines, such as IL-1, IL-2, IL-3, IL-12, interferon-γ (IFN-γ), and GM-CSF. The disease is likely the result of type 3 and type 4 hypersensitivity reactions.
Clinical forms of mold allergy - Hypersensitivity pneumonitis (HP) caused by fungi
The clinical course of this disease widely varies, and its diagnosis is clinically challenging because no specific test or biomarker allows a consistent diagnosis. [13] Therefore, a combination of symptoms, bronchoalveolar lavage findings, chest imaging, laboratory results, and biopsies are needed for an accurate diagnosis.
Regardless of the cause or the responsible environment, the histopathology is similar and usually consists of a granulomatous interstitial bronchiolocentric pneumonitis characterized by the presence of poorly formed granulomas and a prominent interstitial infiltrates composed of lymphocytes, plasma cells, and macrophages. Importantly, patients with chronic HP may evolve to interstitial fibrosis or develop emphysematous changes. Identification of biomarkers that may predict outcome and progression is essential for the success of the treatment.
Epidemiology
Frequency
United States
Depending on patients' geographic locations, their mold allergies can be seasonal (most often fall) or perennial. Perennial mold allergies are prevalent in humid and warm climates secondary to persistent presence of molds in indoor environments. Among preschool aged children living in the southern United States with documented reactivity to indoor allergens, 80% had reactivity to mold spores, house dust mites, or both. No data are available for the prevalence of the 5 other clinical disorders listed in Pathophysiology section. EAA is considered to be more prevalent among workers whose occupations predispose them to repeated exposure to causative reagents.
International
No epidemiologic data are currently available. However, in recent years, mold exposure in schoolchildren has become a major concern of parents and healthcare professionals worldwide. The increase in mold allergy symptoms in susceptible children may be partly attributed to improper repair of moisture-damaged buildings or congested homes of the inner city.
An interesting observation was reported in Poland. [13] A survey of art conservators found that 85% of art conservators and museum workers reported allergic symptoms. Cladosporium, Alternaria, and yeasts were the species that played the most important role in the development of fungal hypersensitivity. A duration of occupational exposure of longer than 5 years, the presence of domestic animals (especially a cat at home), elevated total IgE level, allergic rhinitis, and skin sensitivity to common allergens (eg, grass pollens, mites) are significant risk factors for the development of hypersensitivity to fungi among those museum workers.
Mortality/Morbidity
Anaphylaxis due to a mold allergy is extremely rare, but a mold allergy could cause a severe respiratory reaction if the patient has allergic bronchial asthma due to mold sensitivity. How much mold allergy contributes to mortality in asthma patients is unknown.
Morbidity associated with mold allergy is high in pediatric population because most children develop allergic symptoms early in their lives following exposure to mold allergens.
Although the patient number is limited, those who develop ABPA, ABPM, AFS, or EAA generally experience chronic, relapsing clinical courses. These patients must be aggressively treated during relapse. When ABPA, ABPM, hypersensitive pneumonitis, or EAA is not well controlled, it can result in substantial disability or even death.
The frequency of prolonged coldlike symptoms in winter, sinusitis, and adenoid hypertrophy is higher among the children who have mold allergy than those without mold allergy.
Demographics
Mold allergy is prevalent in all age groups, and it may occur in young children secondary to indoor exposure to mold.
Allergic rhinitis and allergic asthma can occur in children and adults. ABPM and EAA are rare in children. ABPA has been reported in children of all ages, especially in those with CF.
In children with Alternaria-sensitive moderate-to-severe asthma, an increased type 2 helper cell (Th2) sensitivity to Alternaria stimulation was noted. [14] This was associated with a human leukocyte antigen (HLA)-DR restriction, and with increased frequency of HLA-DRB1*13 and HLA-DRB1*03. A decreased frequency of HLA-DQB1*03 was noted in Alternaria -sensitive moderate-to-severe asthma, suggesting HLA-DQB1*03 may be protective to the development.
-
Aspergillus.
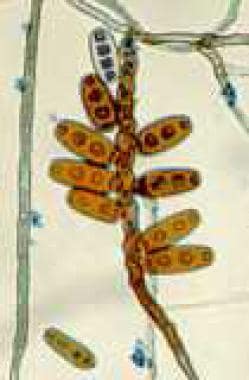
-
Alternaria alternata.
-
Bathrooms are favorite habitats for mold.
-
Moisture is trapped in the wall behind a vinyl wall covering.
-
Large amounts of moisture support fungal growth, as is the case with this dry wall covering.
-
Fungi collected from a spore sampler found in a cubic meter of air.
-
Glues can collect mold.
-
Soapy shower doors collect fungi.
-
Wet drywall collects mold.
-
Wall coverings can pucker because of mold.
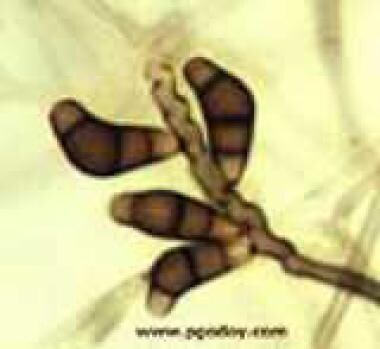
-
Bipolaris.
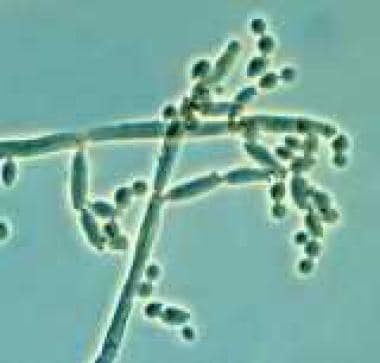
-
Cladosporium (Hormodendrum).
-
Curvularia.
-
Dreschlera (Helminthosporium).
-
Epicoccum.
-
Penicillium.
-
Penicillium.
-
Stachybotrys.
-
Rhizopus.
Tables

What would you like to print?
- Overview
- Presentation
- DDx
- Workup
- Treatment
- Medication
- Medication Summary
- Antihistamines, oral
- Antihistamines with decongestants, oral
- Antihistamine nasal sprays
- Mast-cell stabilizers
- Antihistamine and mast cell stabilizer eye drops
- Corticosteroid nasal sprays
- Corticosteroid oral inhalers
- Bronchodilators, short term
- Inhaled long-acting bronchodilator/corticosteroid combinations
- Systemic corticosteroids
- Leukotriene antagonists/5-lipoxygenase inhibitors
- Theophylline derivatives
- Monoclonal antibodies
- Anticholinergic nasal sprays and oral inhalers
- Show All
- Follow-up
- Questions & Answers
- Media Gallery
- References





