Background
In 1929, Kenneth Mallory and Soma Weiss first described a syndrome characterized by esophageal bleeding caused by a mucosal tear in the esophagus as a result of forceful vomiting or retching. The initial description was associated with alcoholic binging; however, with the advent of endoscopy, Mallory-Weiss tears have been diagnosed in many patients with no antecedent history of alcohol intake. The tear typically occurs after repeated episodes of vomiting or retching, but it may occur after a single incident. [1] Although most written reports of these tears relate to adults, Mallory-Weiss tears also occur in children.
In pediatrics, Mallory-Weiss tears are recognized in children with predisposing medical conditions, including portal hypertension, liver cirrhosis, and severe gastroesophageal reflux disease. The clinical implications in these pediatric patients are noteworthy, especially because these children are predisposed to recurrent upper GI bleeding. [2] The associated risk of morbidity and mortality must also be underscored.
Examples of Mallory-Weiss tears are shown in the images below.
 Mallory-Weiss Syndrome. Typical longitudinal mucosal tear with overlying fibrinous exudate extending from the distal esophagus to the gastric cardia. Courtesy of C.J. Gostout, MD.
Mallory-Weiss Syndrome. Typical longitudinal mucosal tear with overlying fibrinous exudate extending from the distal esophagus to the gastric cardia. Courtesy of C.J. Gostout, MD.
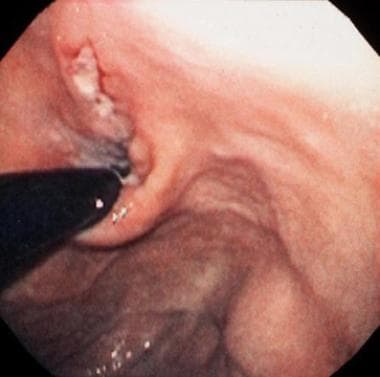 Mallory-Weiss Syndrome. Retroflexed view of the cardia showing the typical location of the tear with a clean base.
Mallory-Weiss Syndrome. Retroflexed view of the cardia showing the typical location of the tear with a clean base.
Pathophysiology
Any disorder that initiates vomiting may result in the development of a Mallory-Weiss tear, which develops as a linear laceration at the gastroesophageal junction because the esophagus and stomach are cylindrical. The cylindrical shape allows longitudinal tears to occur more easily than circumferential tears. These tears have been postulated to occur either by a rapid increase in intragastric pressure and distention, which increases the forceful fluid ejection through the esophagus, or secondary to a significant change in transgastric pressure (ie, difference in pressure across the gastric wall) because negative intrathoracic pressure and positive intragastric pressure leads to distortion of the gastric cardia, resulting in a gastric or esophageal tear. Aside from those patients who present with upper GI bleeding secondary to an alcohol binge, Mallory-Weiss tears occur more commonly in people with hiatal hernias.
Although most cases of Mallory-Weiss tears are self-limiting, patients with severe or recurrent episodes of bleeding that require intensive care therapy and interventional endoscopy have been reported. Typically, these patients have underlying conditions, including portal hypertension and hepatic insufficiency. Although upper GI bleeding is generally assumed to be secondary to varices in these patients, the physician must also be aware of the potential for Mallory-Weiss tears.
Etiology
Many underlying disorders that cause vomiting and retching result in a Mallory-Weiss tear. Gastrointestinal (GI) diseases associated with Mallory-Weiss tears include the following:
-
Ulcers
-
Inflammatory conditions of the stomach and intestine
-
Hepatitis: Acute inflammation of the liver causes vomiting in 10-20% of patients.
-
Biliary tract disease: Although rare in children, these conditions can cause vomiting typically associated with meals and include gallstones, cholecystitis, and biliary cirrhosis.
-
Hyperemesis gravidarum: Some women develop hyperemesis gravidarum, a syndrome characterized by persistent severe vomiting and retching, in the first trimester of pregnancy. Gastric dysrhythmias and prolonged small-bowel motility cause the development of hyperemesis gravidarum. Some women lose as much as 10% of their body weight during this period.
Vomiting is often associated with diseases affecting the kidneys, including the following:
Intracranial lesions that cause hydrocephalus or increased intracranial pressure may lead to vomiting in children. Most common causes of hydrocephalus include tumors, cysts, and congenital abnormalities. Other causes of increased intracranial pressure consist of trauma, infections (eg, meningitis), medications, and pseudotumor cerebri.
Iatrogenic causes of Mallory-Weiss tears include complications of endoscopy resulting in esophageal tears (< 0.01% in children) and are almost always associated with a patient who is retching or struggling during the procedure. The use of polyethylene glycol lavage, when used for ingestions, severe constipation, or preparation for colonoscopy, may cause severe vomiting.
Other causes of vomiting and retching that may result in a Mallory-Weiss tear include the following:
-
Severe diabetic ketoacidosis
-
Toxins
-
Drugs (eg, chemotherapeutic agents)
Epidemiology
United States data
Mallory-Weiss tears cause approximately 3-15% of all episodes of hematemesis in adults; however, these tears are less common in children (< 5% of all upper GI bleeding episodes).
Race-, sex-, and age-related demographics
In a retrospective study of Black and Hispanic patients presenting with upper GI bleeding over a 10-year period, Mallory-Weiss Tear was diagnosed in 84 of 698 of patients. Among these patients, more than half did not have a history of retching or vomiting, and 216 patients presented with hemodynamic instability. Overall, 10% of patients died from a failure to achieve hemostasis and secondary to associated comorbidities. [3]
Mallory-Weiss tears are equally common among male and female children. These tears also occur with equal frequency in both sexes in adults, although they have different causes. In women of childbearing age, the most common cause of these tears is hyperemesis gravidarum, which usually occurs in the first trimester, causing severe persistent nausea and vomiting. Any adolescent female presenting with a Mallory-Weiss tear should be evaluated for pregnancy, as well as bulimia and anorexia nervosa. Furthermore, the potential for drug and alcohol ingestion must also be underscored in the adolescent patient.
Mallory-Weiss tears usually occur in the fifth and sixth decades of life. In children, tears are more commonly observed in older children and adolescents secondary to increased intragastric and transgastric pressures that develop at an older age. However, children with underlying medical conditions, including gastroesophageal reflux and liver disease, can present at any age.
Prognosis
Prognosis is extremely good in children, with a less than 0.01% mortality rate. These tears almost always respond to conservative therapy and supportive care. [4]
Morbidity/mortality
Although children rarely have hemodynamic instability secondary to upper GI bleeding associated with Mallory-Weiss tears, the risk for potential complication, including shock, must be underscored in patients with portal hypertension and hepatic insufficiency.
The major factor in a poor outcome of a Mallory-Weiss tear is bleeding. [5, 6] Patients present with variable bleeding, which can range from a few specks or streaks of blood mixed with mucus to copious amounts of fresh red blood. In adults, shock occurs in as many as 20% of patients bleeding from Mallory-Weiss tears who present to emergency departments; as many as 45% of patients develop postural hypotension. Indeed, studies have also shown that those patients who present clinically in shock are more likely to require intensive care management and interventional endoscopic procedures. Moreover, these patients are more likely to experience recurrent episodes of bleeding secondary to Mallory-Weiss tears. [7]
Predictive factors for recurrent bleeding include the following [8] :
-
Initial presentation of shock: In a study of 159 patients treated for Mallory-Weiss tears, 17 patients (10.7%) experienced recurrent bleeding. Those patients were in shock at initial presentation and had active bleeding on endoscopic evaluation. [9]
-
Liver cirrhosis
-
Decreased hemoglobin and platelet count: In a study of 93 patients who were managed for Mallory-Weiss tears, 9 had a fatal outcome. In that study, multivariant analysis showed that advanced age, a low hemoglobin level at clinical presentation, and the presence of tarry stool were associated with an increased risk of dying. [10]
-
Need for blood transfusion
-
Intensive care management
-
Active bleeding noted at the time of endoscopy
Future studies are necessary to validate these clinical observations, and they may perhaps lead to the development of a measure tool for clinical risk among patients presenting with Mallory-Weiss tears.
Complications
Complications include the following:
-
Anemia
-
Dehydration
-
Mallory-Weiss Syndrome. Typical longitudinal mucosal tear with overlying fibrinous exudate extending from the distal esophagus to the gastric cardia. Courtesy of C.J. Gostout, MD.
-
Mallory-Weiss Syndrome. Retroflexed view of the cardia showing the typical location of the tear with a clean base.





