Practice Essentials
Intussusception (see the image below) is a process in which a segment of intestine invaginates into the adjoining intestinal lumen, causing bowel obstruction. [1] With early diagnosis, appropriate fluid resuscitation, and therapy, the mortality rate from intussusception in children is less than 1%. If left untreated, however, this condition is uniformly fatal in 2-5 days.

History
The patient with intussusception is usually an infant, often one who has had an upper respiratory infection, who presents with the following symptoms:
-
Vomiting: Initially, vomiting is nonbilious and reflexive, but when the intestinal obstruction occurs, vomiting becomes bilious
-
Abdominal pain: Pain in intussusception is colicky, severe, and intermittent
-
Passage of blood and mucus: Parents report the passage of stools, by affected children, that look like currant jelly; this is a mixture of mucus, sloughed mucosa, and shed blood; diarrhea can also be an early sign of intussusception
-
Lethargy: This can be the sole presenting symptom of intussusception, which makes the condition’s diagnosis challenging
-
Palpable abdominal mass
Physical examination
The hallmark physical findings in intussusception are a right hypochondrium sausage-shaped mass and emptiness in the right lower quadrant (Dance sign). This mass is hard to detect and is best palpated between spasms of colic, when the infant is quiet. Abdominal distention frequently is found if the obstruction is complete.
See Clinical Presentation for more detail.
Diagnosis
Imaging studies used in the diagnosis of intussusception include the following:
-
Radiography: Plain abdominal radiography reveals signs that suggest intussusception in only 60% of cases
-
Ultrasonography: Hallmarks of ultrasonography include the target and pseudokidney signs
-
Contrast enema: This is the traditional and most reliable way to make the diagnosis of intussusception in children
See Workup for more detail.
Management
Nonoperative reduction
Therapeutic enemas include the following:
-
Hydrostatic: With barium or water-soluble contrast
-
Pneumatic: With air insufflation; this is the treatment of choice in many institutions, and the risk of major complications with this technique is small
Surgical reduction
Traditional entry into the abdomen is through a right paraumbilical incision. The intussusception is delivered into the wound, and manual reduction is attempted. It is important that the intussusception be milked out of the intussuscipiens.
If manual reduction is not possible or perforation is present, a segmental resection with an end-to-end anastomosis is performed.
Laparoscopy has been added to the surgical armamentarium for intussusception [2, 3] and can be performed in all cases of intussusception.
See Treatment and Medication for more detail.
Background
Intussusception is a process in which a segment of intestine invaginates into the adjoining intestinal lumen, causing bowel obstruction. A common cause of abdominal pain in children, intussusception is suggested readily in pediatric practice based on a classic triad of signs and symptoms: vomiting, abdominal pain, and passage of blood per rectum. (See History and Physical Examination.)
Intussusception presents in 2 variants: idiopathic intussusception, which usually starts at the ileocolic junction and affects infants and toddlers, and enteroenteral intussusception (jejunojejunal, jejunoileal, ileoileal), which occurs in older children. The latter is associated with special medical situations (eg, Henoch-Schönlein purpura [HSP], cystic fibrosis, hematologic dyscrasias) or may be secondary to a lead point and occasionally occur in the postoperative period. Intussusception is demonstrated in the images below. (See Etiology and Pathophysiology.)
 Abdominal radiograph shows small bowel dilatation and paucity of gas in the right lower and upper quadrants.
Abdominal radiograph shows small bowel dilatation and paucity of gas in the right lower and upper quadrants.

 CT scan reveals the classic ying-yang sign of an intussusceptum inside an intussuscipiens.
CT scan reveals the classic ying-yang sign of an intussusceptum inside an intussuscipiens.
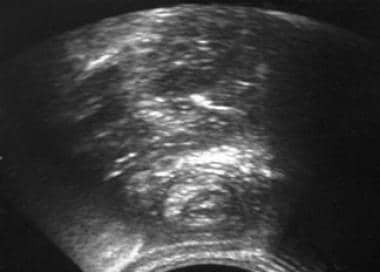 Abdominal ultrasonography reveals the classic target sign of an intussusceptum inside an intussuscipiens.
Abdominal ultrasonography reveals the classic target sign of an intussusceptum inside an intussuscipiens.

Go to Pediatric Intussusception Surgery for complete information on this topic.
Patient education
Educate parents and caregivers of a patient treated with nonoperative reduction with regard to the risks and signs and symptoms of recurrence so that the initiation of care is not delayed.
Etiology and Pathophysiology
The pathogenesis of idiopathic intussusception is not well established. It is believed to be secondary to an imbalance in the longitudinal forces along the intestinal wall. In enteroenteral intussusception, this imbalance can be caused by a mass acting as a lead point or by a disorganized pattern of peristalsis (eg, an ileus in the postoperative period).
As a result of imbalance in the forces of the intestinal wall, an area of the intestine invaginates into the lumen of adjacent bowel. The invaginating portion of the intestine (ie, the intussusceptum) completely “telescopes” into the receiving portion of the intestine (ie, the intussuscipiens). This process continues and more proximal areas follow, allowing the intussusceptum to proceed along the lumen of the intussuscipiens.
If the mesentery of the intussusceptum is lax and the progression is rapid, the intussusceptum can proceed to the distal colon or sigmoid and even prolapse out the anus. The mesentery of the intussusceptum is invaginated with the intestine, leading to the classic pathophysiologic process of any bowel obstruction.
Early in this process, lymphatic return is impeded; then, with increased pressure within the wall of the intussusceptum, venous drainage is impaired. If the obstructive process continues, the pressure reaches a point at which arterial inflow is inhibited, and infarction ensues. The intestinal mucosa is extremely sensitive to ischemia because it is farthest away from the arterial supply. Ischemic mucosa sloughs off, leading to the heme-positive stools and subsequently to the classic "currant jelly stool" (a mixture of sloughed mucosa, blood, and mucus). If untreated, transmural gangrene and perforation of the leading edge of the intussusceptum occur.
Lead points
In approximately 2-12% of children with intussusception, a surgical lead point is found. Occurrence of surgical lead points increases with age and indicates that the probability of nonoperative reduction is highly unlikely. Examples of lead points are as follows:
-
Meckel diverticulum [4]
-
Enlarged mesenteric lymph node
-
Benign or malignant tumors of the mesentery or of the intestine, including lymphoma, polyps, ganglioneuroma, [5] and hamartomas associated with Peutz-Jeghers syndrome
-
Mesenteric or duplication cysts
-
Submucosal hematomas, which can occur in patients with HSP and coagulation dyscrasias
-
Ectopic pancreatic and gastric rests
-
Inverted appendiceal stumps
-
Sutures and staples along an anastomosis
-
Intestinal hematomas secondary to abdominal trauma
-
Foreign body
-
Hemangioma
-
Post-transplantation lymphoproliferative disorder (PTLD) [7]
Henoch-Schönlein purpura
Children with HSP often present with abdominal pain secondary to vasculitis in the mesenteric, pancreatic, and intestinal circulation. If pain precedes cutaneous manifestations, differentiating HSP from appendicitis, gastroenteritis, intussusception, or other causes of abdominal pain is difficult.
Occasionally, children with HSP develop submucosal hematomas, which can act as lead points and cause small bowel intussusception. Elucidating the cause of the pain is essential in any child in whom HSP is suspected.
Since the intussusception associated with HSP is usually enteroenteral (small bowel to small bowel), these patients require surgery rather than an enema.
During the initial investigation, obtain supine and upright plain radiographs of the abdomen to identify the small bowel obstruction associated with intussusception. If radiographic findings are normal, assume the patient with HSP has mesenteric vasculitis and treat with steroids.
Hemophilia and other coagulation disorders
Patients with hemophilia and other bleeding disorders may develop intestinal submucosal hematomas, leading to intussusception. Differential diagnosis includes retroperitoneal hemorrhage in addition to other usual causes of abdominal pain. Radiographs of the abdomen should reveal a pattern of small bowel obstruction if intussusception is present. In the absence of intussusception, treatment is supportive with correction of coagulopathy.
Postoperative intussusceptions
Intussusception is a rare postoperative complication, occurring in 0.08-0.5% of laparotomies. It can take place independently of the site of the operation. The likely mechanism is due to a difference in activity between segments of the intestine recovering from an ileus, which produces the intussusception. [8] Intussusception is suggested in any postoperative patient who has a sudden onset of a small bowel obstruction after a period of ileus, usually within the first 2 weeks after surgery. Intestinal obstruction secondary to adhesions usually occurs more than 2 weeks after the operation. The treatment is prompt operative reduction.
Indwelling catheters
Very rarely, indwelling jejunal catheters can lead to intussusception by acting as a lead point, which is especially true if the tip of the catheter has been manipulated or cut so that its surface is not smooth. The clinical picture is that of a small bowel obstruction. Diagnosis can be facilitated by injecting contrast proximal to the catheter and then through the tip of the catheter. Surgery is required to remove the tip of the catheter and to reduce the intussusception.
Cystic fibrosis
Intussusception occurs in approximately 1% of patients with cystic fibrosis. Intussusception is assumed to be precipitated by the thick, inspissated stool material that adheres to the mucosa and acts as a lead point. Often, the course is indolent and chronic. Differential diagnosis includes distal intestinal obstruction syndrome and appendicitis. The majority of these patients require operative reduction.
Other causes
Electrolyte derangements associated with various medical conditions can produce aberrant intestinal motility, leading to enteroenteral intussusception.
Experimental studies in animals showed that abnormal intestinal release of nitric oxide, an inhibitory neurotransmitter, caused relaxation of the ileocecal valve, predisposing to ileocecal intussusception. [9] Other studies have demonstrated that certain antibiotics cause ileal lymphoid hyperplasia and intestinal dysmotility, with resultant intussusception.
A viral etiology has also been implicated. A seasonal variation in the incidence of intussusception that corresponds to the peaks in frequency of gastroenteritis (spring and summer) and respiratory illnesses (midwinter) has been described. Lappalainen et al have studied prospectively the role of viral infections in the pathogenesis of intussusception. They concluded that the simultaneous presence of human herpesvirus-6 and adenovirus infections appeared to correlate with risk for intussusception. [10]
An association was found between the administration of a rotavirus vaccine (RotaShield) and the development of intussusception. [11] RotaShield has since been removed from the market. These patients were younger than usual for idiopathic intussusception and were more likely to require operative reduction. It was hypothesized that the vaccine caused reactive lymphoid hyperplasia, which acted as a lead point.
In February 2006, a new rotavirus vaccine [RotaTeq] was approved by the US Food and Drug Administration [FDA]. RotaTeq did not show an increased risk for intussusception compared with placebo in clinical trials. [12] A study that involved more than 63,000 patients who received Rotarix or placebo at ages 2 and 4 months reported a decreased risk for intussusception in those patients receiving Rotarix. [13] However, a 2015 study reported that there was a small increase in the risk of intussusception hospitalizations in infants in California since the introduction of rotavirus vaccines, RotaTeq (2006) and Rotarix (2008). [14, 15]
A study by Tate et al that analyzed the intussusception hospitalization rates before (2000–2005) and after (2007–2013) rotavirus vaccine introduction reported that when compared to the prevaccine baseline (11.7 per 100,000), the intussusception hospitalization rate significantly increased by 46% to 101% (16.7-22.9 per 100,000) in children 8-11 weeks of age in the years after the rotavirus vaccine was introduced. No significant change in hospitalization rates were seen in children < 12 months of age and in children 15-24 weeks and 25-34 weeks of age. [16]
Analysis of data from the Kid’s Inpatient Database in the United States has shown a lower than expected rate of hospital discharges for intussusception in infants since the reintroduction of the rotavirus vaccine in 2006. [17]
Familial occurrence of intussusception has been reported in a few cases. Intussusception in dizygotic twins has also been described; however, these reports are extremely rare.
Idiopathic
In most infants and toddlers with intussusception, the etiology is unclear. This group is believed to have idiopathic intussusception. One theory to explain the possible etiology of idiopathic intussusception is that it occurs because of an enlarged Peyer patch; this hypothesis is derived from 3 observations: (1) often, the illness is preceded by an upper respiratory infection, (2) the ileocolic region has the highest concentration of lymph nodes in the mesentery, and (3) enlarged lymph nodes are often observed in patients who require surgery. Whether the enlarged Peyer patch is a reaction to the intussusception or a cause of it is unclear.
Epidemiology
A wide geographic variation in incidence of intussusception among countries and cities within countries makes determining a true prevalence of the disease difficult. Studies on the absolute prevalence of intussusception in the United States are not available. Its estimated incidence is approximately 1 case per 2000 live births. In Great Britain, incidence varies from 1.6-4 cases per 1000 live births.
Overall, the male-to-female ratio is approximately 3:1. With advancing age, gender difference becomes marked; in patients older than 4 years, the male-to-female ratio is 8:1.
Two thirds of children with intussusception are younger than 1 year; most commonly, intussusception occurs in infants aged 5-10 months. Intussusception is the most common cause of intestinal obstruction in patients aged 5 months to 3 years.
Intussusception can account for as many as 25% of abdominal surgical emergencies in children younger than 5 years, exceeding the incidence of appendicitis. Although extremely rare, intussusception has been reported in the neonatal period.
Prognosis
The prognosis in patients with intussusception is excellent if the condition is diagnosed and treated early; otherwise, severe complications and death may occur.
The recurrence rate of intussusception after nonoperative reduction is usually less than 10% but has been reported to be as high as 15%. [18] Most intussusceptions recur within 72 hours of the initial event; however, recurrences have been reported as long as 36 months later. More than 1 recurrence suggests the presence of a lead point. A recurrence is usually heralded by the onset of the same symptoms as appeared during the initial event. [19] Provide similar treatment for a recurrence unless the suggestion of a lead point is very strong (in which case, surgical exploration should be contemplated).
The recurrence rates after air enema and barium enema are 4% and 10%, respectively. Recurrences respond to nonoperative reduction in almost 95% of cases.
Complications associated with intussusception, which rarely occur when the diagnosis is prompt, include the following:
-
Perforation during nonoperative reduction
-
Wound infection
-
Internal hernias and adhesions causing intestinal obstruction
-
Sepsis from undetected peritonitis (major complication from a missed diagnosis)
-
Intestinal hemorrhage
-
Necrosis and bowel perforation
-
Recurrence
With early diagnosis, appropriate fluid resuscitation, and therapy, the mortality rate from intussusception in children is less than 1%. If left untreated, this condition is uniformly fatal in 2-5 days.
-
Abdominal radiograph shows small bowel dilatation and paucity of gas in the right lower and upper quadrants.
-
Air contrast enema shows intussusception in the cecum.
-
Barium enema shows intussusception in the descending colon.
-
CT scan reveals the classic ying-yang sign of an intussusceptum inside an intussuscipiens.
-
Abdominal ultrasonography reveals the classic target sign of an intussusceptum inside an intussuscipiens.
-
Laparoscopic view of a jejuno-jejunal intussusception.
-
Note intussusception in the left upper quadrant on this plain film of an infant with pain vomiting. Courtesy of Kelley W Marshall, MD, Children's Healthcare of Atlanta, Emory University School of Medicine.
-
Intussusception evident during air contrast enema prior to reduction. Courtesy of Kelley W Marshall, MD, Children's Healthcare of Atlanta, Emory University School of Medicine.






