Practice Essentials
The family Campylobacteraceae includes 2 genera: Campylobacter and Arcobacter. The genus Campylobacter includes 18 species and subspecies; 11 of these are considered pathogenic to humans and cause enteric and extraintestinal illnesses. The major pathogens are Campylobacter jejuni (see the image below) and Campylobacter fetus. [1]
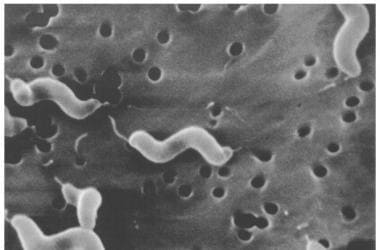 Scanning electron microscope image of Campylobacter jejuni, illustrating its corkscrew appearance and bipolar flagella. Source: Virginia-Maryland Regional College of Veterinary Medicine, Blacksburg, Virginia.
Scanning electron microscope image of Campylobacter jejuni, illustrating its corkscrew appearance and bipolar flagella. Source: Virginia-Maryland Regional College of Veterinary Medicine, Blacksburg, Virginia.
The following Campylobacter species and subspecies are pathogenic to humans:
-
Enteric
C jejuni subspecies jejuni
C jejuni subspecies doylei
Campylobacter coli
Campylobacter upsaliensis
Campylobacter lari
C fetus subspecies fetus
Campylobacter hyointestinalis
Campylobacter concisus
-
Extraintestinal
C jejuni subspecies jejuni
C upsaliensis
C lari
C fetus subspecies fetus
C concisus
Campylobacter sputorum
Campylobacter curvus
Campylobacter rectus
Campylobacter pylori has been reclassified as Helicobacter pylori and is not addressed in this article (see Helicobacter Pylori Infection).
Campylobacter pathogens are small, curved, motile, microaerophilic, gram-negative rods. They vary in width from 0.2-0.9 mm and vary in length from 0.5-5.0 mm. They exhibit rapid, darting motility in corkscrew fashion using a single flagellum or 2 flagella (monotrichous, amphitrichous). They also possess a lipopolysaccharide endotoxin.
Campylobacteriosis infects humans and animals. The animal reservoir is the gastrointestinal tract of dogs, cats, and other pets that can carry the organism. Transmission of C jejuni to humans occurs by ingestion of contaminated food or water, including unpasteurized milk and undercooked poultry, or by direct contact with fecal material from infected animals or persons. The 2 types of illnesses associated with Campylobacter infections in humans are intestinal infection and extraintestinal infection. The prototype for intestinal infection is C jejuni, and the prototype for extraintestinal infection is C fetus.
Pathophysiology
Factors responsible for the diseases caused by C jejuni are not well known. Based on clinical illness, researchers have postulated the following mechanisms [2] :
-
Adherence and production of heat-labile enterotoxins, inducing secretory diarrhea
-
Invasion and proliferation within the intestinal epithelium, leading to cell damage and inflammatory response
-
Translocation of the organism into the intestinal mucosa and proliferation in the lamina propria and mesenteric lymph nodes, leading to extraintestinal infections such as meningitis, cholecystitis, urinary tract infection, and mesenteric adenitis
Information on the pathogenesis of Campylobacter infections other than C jejuni is scarce. Bacteremia is more common with C fetus infection. A surface protein in C fetus inhibits the C3b binding responsible for both the serum and phagocytic resistance of the organism, making the organism resistant to the bactericidal effects of human serum. After oral ingestion, C fetus may colonize the intestinal tract, resulting in portal bacteremia. In immunocompetent hosts, the organism is phagocytosed by the reticuloendothelial cells in the liver, preventing further spread. However, in patients that have predisposing factors that might serve as a local site of infection such as a gravid uterus, bacteremia can lead to severe complications. Infants may be affected hematogenously or by ascending infection during amnionitis and premature rupture of membranes.
Etiology
Individuals at increased risk for Campylobacter enteritis include the following:
-
Those with occupational exposure to cattle, sheep, and other farm animals [3]
-
Laboratory workers
-
Those in contact with the excreta of infected persons
-
Homosexual men
The following underlying conditions increase risk for Campylobacter bacteremia, suggesting the importance of both humoral and cell-mediated immunity [4, 5, 6] :
-
Hypogammaglobulinemia
-
Kwashiorkor
-
Pregnancy
-
Malignancy
-
Extremes of age
-
Alcoholism
-
Diabetes mellitus
-
Postsplenectomy status
-
Human leukocyte antigen B27 (HLA-B27) - Increases risk for immunoreactive complications, such as reactive arthritis or Reiter syndrome
Epidemiology
United States statistics
In the United States, 2 million symptomatic enteric Campylobacter infections are estimated per year (1% of the US population per year). [7] Incidence in the rural population is 5-6 times higher because of increased consumption of raw milk. Among all age groups, the highest incidence occurred among children younger than 5 years; hospitalization occurred in 927 of cases (4.6%), and 8 individuals died. [8] According to the Foodborne Diseases Active Surveillance Network (FoodNet) of the Centers for Diseases Control and Prevention (CDC) which collects data on the incidence of infection with foodborne pathogens, in 2017, 9421 cases of laboratory-confirmed (by isolation of bacteria from a clinical specimen by culture or by culture- independent diagnostics tests) Campylobacter infections were reported in the United States with an overall incidence rate of 19.1 cases per 100,000 population. This was a 10% increase compared to 2014-2016. [9]
For 2022, FoodNet reported that the incidence of Campylobacter infection in the United States was 19.2 cases per 100,000 population. The incidence is similar to the average annual incidences during 2016-2018. [10]
International statistics
In developing and developed countries, continuous increases in the number of C jejuni infections have been seen, with incidence rates as high as 73 cases per 100,000 population reported. [11]
In England and Wales, an increase of laboratory confirmed Campylobacter cases was noted, from 44,544 per year in 2004 to 64,582 per year in 2011. Between 2004 and 2011, a 36% increase of cases occurred among children younter than 10 years, a 25% increase occurred among persons aged 10-45 years, and an 81% increase occurred among those aged 50 years and older. [12]
Overall, Campylobacter gastroenteritis is still common during the first 5 years of life. [13, 14, 15] Isolation rates in children with acute diarrhea range from 10-46%. [13, 15, 16]
Race-, sex-, and age-related demographics
Race
Campylobacter infection has no race predilection.
Sex
In England and Wales, incidence was higher in males from birth until age 17 years and in females aged 20-36 years. [17]
Age
Individuals of any age can be infected with C jejuni enteritis. The rate of infection differs between developed and developing countries. In developed countries, the peak attack rates are in infants younger than 1 year; a second, broader peak attack rate occurs in persons aged 20-29 years. [18] In developing countries, symptomatic infection chiefly affects children younger than 5 years and declines with age. [19, 20] This is likely due to the development of protective immunity secondary to a high level of exposure to the organism early in life.
A study in Bangladesh found that Campylobacter infection is very common during the first 2 years of life. Many of the cases are asymptomatic. [21]
In contrast to the age-specific distribution of Campylobacter enteritis, the highest rate of bacteremia occurs in patients aged 69 years and older. [4] Roughly 30% of isolates are C jejuni, 9% are C coli, and 53% are C fetus.
Prognosis
Most patients fully recover after C jejuni infection, with or without antibiotics.
Campylobacter septicemia in patients with immune deficiencies (including congenital hypogammaglobulinemia, acquired hypogammaglobulinemia, malnutrition, HIV) and in neonates is associated with a high mortality rate.
Even with plasmapheresis and intravenous immunoglobulin, as many as 20% of patients with Guillain-Barré syndrome (GBS) may require mechanical ventilation. Between 15% and 20% of all patients may develop severe neurologic deficit. GBS disease may result in mortality in 5-10% of all patients. Because GBS secondary to C jejuni may be more severe, the number of patients who require mechanical ventilation, experience severe neurologic sequelae, and die may also be higher.
Previously healthy persons infected with C fetus usually recover without sequelae. This infection may be lethal to patients with altered immune status and neonates. Prognosis for these patients depends on the early administration of fluids and appropriate antimicrobial therapy.
Morbidity/mortality
The vast majority of patients fully recover from C jejuni infection within 5 days (range, 2-10 d), either spontaneously or after appropriate antimicrobial therapy. Infection with C fetus is a concern in immunocompromised patients, pregnant women, and neonates. Previously healthy patients usually recover without complications.
Complications
Guillain-Barré syndrome
GBS is a disorder of peripheral nerves and is characterized by ascending paralysis.
Strong evidence suggests an association between preceding C jejuni infection and GBS. [22] The antigenic similarity between specific regions (terminal tetrasaccharide) of lipopolysaccharide of C jejuni and human gangliosides (GM1) led to the concept of molecular mimicry. [23] This concept implies the sharing of homologous epitopes between the bacterial lipopolysaccharide and ganglioside surface components of the peripheral nerve. Immune response from simple C jejuni infection could induce antibodies that cross-react to the gangliosides and trigger GBS.
Other variants of GBS associated with C jejuni infection include the following:
-
Acute motor axonal neuropathy (AMAN), or Chinese paralytic syndrome, is characterized by a rapid onset of paralysis with progression to tetraplegia and respiratory failure and occurs in children in northern China during summer and fall. [24]
-
Fisher syndrome is characterized by ophthalmoplegia, areflexia, and cerebellar ataxia.
Reactive arthritis
Incidence and prevalence of Campylobacter-associated reactive arthritis varies among different reports, ranging from 0.6-24%. [25, 26]
Development of reactive arthritis has been associated with human leukocyte antigen (HLA)-B27 allele; in these individuals, the disease is more severe than in individuals without HLA-B27. [27] However, a more recent population-based study did not show the association. [28]
Arthritis starts a few days to several weeks after the episode of diarrhea. The course is usually self-limited, ranging from 1 week to several months (< 6 mo). [25]
Other infrequently reported complications are as follows:
-
Reiter syndrome
-
Hepatitis
-
Intestinal nephritis
Patient Education
Tips for preventing campylobacteriosis
Thoroughly cook all poultry products. If served undercooked poultry in a restaurant, return it for further cooking.
Wash hands with soap before and after handling raw foods of animal origin.
Prevent cross-contamination in the kitchen as follows:
-
Use separate cutting boards for foods of animal origin and other foods.
-
Carefully clean all cutting boards, countertops, and utensils with soap and hot water after preparing raw food of animal origin.
Avoid consuming unpasteurized milk [29] and untreated surface water. [30]
Make sure that persons with diarrhea, especially children, carefully and frequently wash their hands with soap to reduce the risk of spreading infection.
Wash hands with soap after contact with pet feces.
-
Scanning electron microscope image of Campylobacter jejuni, illustrating its corkscrew appearance and bipolar flagella. Source: Virginia-Maryland Regional College of Veterinary Medicine, Blacksburg, Virginia.





