Practice Essentials
Diabetic ketoacidosis (DKA) in children is defined as a blood glucose level over 11 mmol/L, venous pH below 7.3 or serum bicarbonate level below 15 mmol/L, and either the presence of ketonemia (blood β-hydroxybutyrate level ≥ 3 mmol/L) or moderate to high ketonuria. [1]
In pediatric and adult cases, this condition is a metabolic derangement caused by the absolute or relative deficiency of the anabolic hormone insulin. Together with the major complication of cerebral edema, it is the most important cause of mortality and severe morbidity in children with diabetes.
Signs and symptoms
Symptoms of acidosis and dehydration include the following:
-
Abdominal pain - May be severe enough to present as a surgical emergency
-
Shortness of breath - May be mistaken for primary respiratory distress
-
Confusion and coma in the absence of recognized head injury [2]
Symptoms of hyperglycemia, a consequence of insulin deficiency, include the following:
-
Polyuria - Increased volume and frequency of urination
-
Polydipsia - Thirst is often extreme
-
Nocturia and secondary enuresis in a previously continent child
-
Weight loss - May be dramatic due to breakdown of protein and fat stores
-
Muscle pains and cramps
Patients with diabetic ketoacidosis may also have the following signs and symptoms:
-
Vomiting
-
Dehydration
-
Signs of intercurrent infection (eg, urinary or respiratory tract infection)
-
Weakness and nonspecific malaise that may precede other symptoms of hyperglycemia
-
Tachycardia
-
Reduced capillary refill
-
Kussmaul breathing or deep sighing respiration - A mark of acidosis
-
Ketone odor - Patient may have a smell of ketones on his/her breath
-
Impaired consciousness - Occurs in approximately 20% of patients
-
Coma - May be present in 10% of patients
-
Abdominal tenderness - Usually nonspecific or epigastric in location
Cerebral edema
Most cases of cerebral edema occur 4-12 hours after initiation of treatment. Diagnostic criteria of cerebral edema include the following:
-
Abnormal motor or verbal response to pain
-
Decorticate or decerebrate posture
-
Cranial nerve palsy - Especially III, IV, and VI
-
Abnormal neurogenic breathing pattern (eg, Cheyne-Stokes), apneusis
Major criteria include the following:
-
Altered mentation, fluctuating level of consciousness
-
Sustained and inappropriate bradycardia
-
Age-inappropriate incontinence
Minor criteria include the following:
-
Vomiting
-
Headache
-
Abnormal drowsiness
-
Diastolic hypertension (>90 mm Hg)
See Clinical Presentation for more detail.
Diagnosis
Laboratory studies
The following lab studies are indicated in patients with diabetic ketoacidosis:
-
Blood glucose
-
Blood gases
-
Potassium
-
Sodium
-
Blood urea and creatinine
-
Bicarbonate - Usually available from blood gas analysis
-
Capillary blood ketone
-
Glycosylated hemoglobin (HbA1c)
-
Full blood count
-
Urine
-
Insulin
-
Culture
-
Amylase
-
Serum osmolarity
-
Phosphate, calcium, and magnesium
-
Lipids
Imaging studies
-
Head computed tomography (CT) scanning - If coma is present or develops
-
Chest radiography - If clinically indicated
Electrocardiography
Electrocardiography (ECG) is a useful adjunct to monitor potassium status. Characteristic changes appear with extremes of potassium status. See the images below.
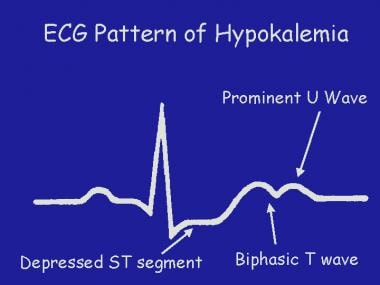 Pediatric Diabetic Ketoacidosis. A graphical representation of the electrocardiographic changes of hypokalemia.
Pediatric Diabetic Ketoacidosis. A graphical representation of the electrocardiographic changes of hypokalemia.
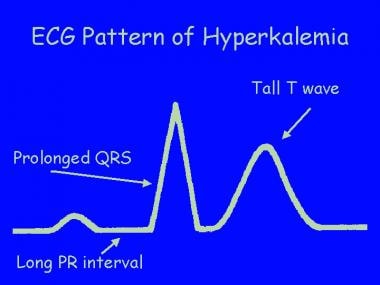 Pediatric Diabetic Ketoacidosis. A graphical representation of the electrocardiographic changes of hyperkalemia (due to overcorrection of potassium loss).
Pediatric Diabetic Ketoacidosis. A graphical representation of the electrocardiographic changes of hyperkalemia (due to overcorrection of potassium loss).
Consciousness
Check the patient’s consciousness level hourly for up to 12 hours, especially in a young child with a first presentation of diabetes. The Glasgow coma scale is recommended for this purpose.
See Workup for more detail.
Management
Replacement of the following is essential in the treatment of diabetic ketoacidosis:
-
Fluid - Published series suggest that the best outcomes have been achieved by using isotonic sodium chloride solution or half-strength sodium chloride solution for first resuscitation and replacement [3]
-
Insulin - Continuous, low-dose, intravenous (IV) insulin infusion is generally considered the safest and most effective insulin delivery method for diabetic ketoacidosis
-
Potassium - After initial resuscitation and if serum/plasma levels are below 5 mEq/L or a good renal output has been maintained, add potassium to all replacement fluids
-
Bicarbonate - Used only in select cases; the only justification for using IV bicarbonate is acidosis sufficiently severe to compromise cardiac contractility
Cerebral edema
If cerebral edema is suspected and hypoglycemia is excluded, prompt treatment with an osmotic diuretic is indicated, followed by a CT scan and referral to a neurosurgeon. Intubation, hyperventilation, and intracranial pressure monitoring reportedly improve outcomes.
See Treatment and Medication for more detail.
Background
Diabetic ketoacidosis (DKA) in children is defined as a blood glucose level over 11 mmol/L, venous pH below 7.3 or serum bicarbonate level below 15 mmol/L, and either the presence of ketonemia (blood β-hydroxybutyrate level ≥ 3 mmol/L) or moderate to high ketonuria. [1]
This condition, together with the major complication of cerebral edema, is the most important cause of mortality and severe morbidity in pediatric cases of diabetes, particularly at the time of first diagnosis. (See Pathophysiology and Prognosis.)
Early recognition and careful management of ketoacidosis—a metabolic derangement caused by the absolute or relative deficiency of the anabolic hormone insulin—are essential if death and disability are to be avoided. (See Pathophysiology, Etiology, Presentation, Workup, Treatment, and Medication.) [4]
Patient education
For patient education information, see the Diabetes Center, as well as Diabetic Ketoacidosis.
Pathophysiology
Insulin is the pivotal hormone of blood glucose regulation, increasing peripheral glucose uptake and switching off hepatic gluconeogenesis, while stimulating glycogen synthesis and peripheral fat deposition.
Insulin deficiency exaggerates the normal response to fasting, which is to increase liver production of glucose by gluconeogenesis from fat and protein together with the breakdown of liver glycogen stores by glycogenolysis. Peripheral glucose uptake is impaired and levels of the main counterregulatory hormones (ie, glucagon, cortisol, catecholamines, growth hormone) increase. Various metabolic consequences follow. [5]
Hyperglycemia
Glucagon stimulates glycogenolysis and gluconeogenesis, doubling liver glucose production. Hyperglycemia further impairs peripheral glucose uptake and inhibits any residual insulin synthesis. Blood glucose levels rise above the renal threshold for glucose reabsorption, causing an osmotic diuresis.
Fluid and electrolytes
Although they tend to be overestimated, fluid losses can be considerable, typically reaching 3-8% of body weight. [6] Most water is lost by osmotic diuresis, with important contributions from hyperventilation and vomiting. The diuresis also leads to significant urinary losses of potassium, sodium, phosphate, and magnesium ions.
Ketoacidosis
Insulin inhibits the lipolytic action of cortisol and growth hormone; thus, insulin deficiency increases circulating levels of fatty acids. These are oxidized in the liver, producing the acidic ketone bodies beta hydroxybutyrate and acetoacetate, from which acetone spontaneously forms. The resulting acidosis primarily is due to circulating ketone bodies, with additional contributions from excess fatty acids and lactic acidosis, as a consequence of poor tissue perfusion.
Eventually, hyperventilation no longer can compensate for the metabolic acidosis, which, together with dehydration, leads to renal failure and circulatory collapse, followed by coma and death.
Cerebral edema
The cause of cerebral edema associated with diabetic ketoacidosis is unknown, but associated factors include duration and severity of diabetic ketoacidosis before treatment, overaggressive fluid replacement, the use of sodium bicarbonate to treat the acidosis, too early an introduction of insulin therapy, cerebral anoxia, and degree of hyperglycemia. [7, 8, 9, 10, 11, 12]
Various theories have been offered to explain cerebral edema’s pathogenesis in diabetic ketoacidosis.
A widely accepted hypothesis suggests that cerebral edema results from ischemia-reperfusion injury, with inflammation and impaired cerebrovascular autoregulation playing a role in the pathogenesis. [12] Similary, some researchers propose cerebral edema develops secondary to cerebral ischemia caused by hypocapnia, dehydration, and hyperglycemia. [13] This explains why some children present with cerebral edema before treatment and most known factors (eg, severity of hypocapnia, acidosis, dehydration, duration of ketoacidosis). Cerebral imaging studies of children with diabetic ketoacidosis and animal models make this the most compelling theory and offer an opportunity to actively prevent or better treat cerebral edema developing with ketoacidosis. [13]
Another theory postulates that brain cells produce idiogenic osmoles to prevent cell shrinkage in a hyperosmolar environment. These osmoles are slow to clear from the cells, and as plasma osmolarity falls during treatment, water is drawn into the brain cells by the resulting osmotic gradient. This accounts for the belief that overrapid correction of hyperosmolarity is associated with cerebral edema.
A third theory proposes an effect on the cell membrane sodium/hydrogen transport system. As diabetic ketoacidosis develops, acidic molecules accumulate in intracellular and extracellular fluids. With treatment, the concentration of acid falls more rapidly in the extracellular compartment, causing a net influx of sodium and water into the cells as hydrogen ions are exchanged. This may explain why cerebral edema seems to appear with biochemical correction of acidosis.
Etiology
Twenty-five percent of patients with a new diagnosis of diabetes present with diabetic ketoacidosis; a missed diagnosis of diabetes is the most common cause, especially in young children.
In children with established diabetes, the causes of diabetic ketoacidosis vary with age. Infection is the most likely precipitant in the prepubertal child; missed injections or emotional upset are more usual in the older teenager.
Failure to administer prescribed insulin is the most common cause of diabetic ketoacidosis in adolescents. [14, 15] Children with high glycosylated hemoglobin (HbA1c) levels (a measure of control over an 8- to 12-wk period) may be receiving only a third or less of the prescribed insulin dose. [16] Total insulin deficiency obviously leads to diabetic ketoacidosis, but inadequate doses render the child more liable to decompensate with other stresses such as infection, emotional turmoil, or food bingeing. [17]
Children on continuous subcutaneous insulin infusion are at particular risk of diabetic ketoacidosis if the device fails or if insulin delivery is disrupted, because they have no effective depot of insulin and become insulin-deficient very quickly. Diabetic ketoacidosis is most likely to occur in the first year after commencing continuous subcutaneous insulin infusion. Children with diabetic ketoacidosis often present with vomiting and abdominal pain, symptoms that are mistaken for gastroenteritis or food poisoning.
Children using only analogue insulins are also at risk of rapid-onset diabetic ketoacidosis. Omitting an evening dose of long-acting insulin may result in insulin deficiency through the night and typically leads to the child waking up vomiting.
Some children have repeated episodes of diabetic ketoacidosis (so-called brittle diabetics). These children usually have major emotional disturbances relating to home, school, or relationships with their peer group. They may repeatedly present in a critical condition but invariably deny any failure of compliance. Helping these children is extremely difficult.
Alcohol and drug abuse, particularly with cocaine, amphetamine derivatives, and their analogues, are other precipitants of diabetic ketoacidosis. [18]
In the developing world, infection and the lack of available insulin are the most important causes of diabetic ketoacidosis.
Epidemiology
Exact figures for the incidence of diabetic ketoacidosis are not available. The estimated incidence of diabetic ketoacidosis in pediatric type 1 diabetes mellitus in resource-rich countries appears to be 1-10% per year.
Occurrence in the United States
An estimated one third of children present with diabetic ketoacidosis at diagnosis of type 1 diabetes. [1] A multicenter, population-based study reported that around 25% of new cases of type I diabetes mellitus presented with ketoacidosis, resulting in an approximate annual incidence of 4 cases per 100,000 children. [19] The youngest children were at the greatest risk, with more than 37% presenting with diabetic ketoacidosis. The rates for children with established diabetes increase with age. [20, 21]
International occurrence
As in the United States, few data are available on the incidence of diabetic ketoacidosis. A large, multicenter European study showed widely varying rates of diabetic ketoacidosis at diagnosis (26-67%), with rates inversely related to the overall incidence of childhood diabetes. [22] Diabetic ketoacidosis rates in children with established diabetes widely vary; in a United Kingdom national prospective study, 60% of all cases occurred in patients with known diabetes. [23, 24] Diabetic ketoacidosis at the time of diagnosis is more likely in the most deprived communities.
A 2011 study analyzing 46 published reports [25] reinforced the above statements. The groups most likely to present with diabetic ketoacidosis at diagnosis were the youngest children, particularly those younger than 2 years, and children from the most deprived communities, including children from ethnic minorities or without health insurance. Factors protecting against diabetic ketoacidosis at diagnosis were having a first-degree relative with type 1 diabetes, having better-educated parents, and living in a community with a high background incidence of childhood diabetes.
A multicenter study from Germany and Austria, using a database containing information on 28,770 children aged 19 years or younger, reported that the greatest risk of diabetic ketoacidosis in established cases of type 1 diabetes was in the early teenage years. This was particularly the case in girls and in children from immigrant families. [26]
Race-, sex-, and age-related demographics
Race alone does not appear to have any influence on the likelihood of developing diabetic ketoacidosis, [27] but immigrant communities may be at a higher risk of problems in established cases. [26]
Although no difference in diabetic ketoacidosis rates between the sexes is observed at diagnosis and during early childhood, adolescent girls with diabetes are more likely to develop diabetic ketoacidosis than adolescent boys. [26, 28]
Infants and children younger than 5 years are at the greatest risk of presenting with diabetic ketoacidosis because the diagnosis of diabetes in younger children is more difficult and is more likely to be delayed. [25, 29] Adolescents are more likely to develop diabetic ketoacidosis after the diagnosis of diabetes.
Prognosis
Expect full recovery with appropriate management of diabetic ketoacidosis. The degree and quality of monitoring are probably the most important factors in determining outcomes. However, even if cerebral edema has not occurred, a risk of long-term intellectual deficit is noted in children who have had an episode of diabetic ketoacidosis. [30]
Morbidity and mortality
Diabetic ketoacidosis is the most common cause of diabetes-related death in childhood. Without insulin therapy, the mortality rate is 100%, but current mortality rates are around 2-5%. [31, 32, 33]
Treatment for diabetic ketoacidosis may cause life-threatening, predictable, and avoidable acute complications such as hypokalemia, hypoglycemia, hyponatremia, and fluid overload. Other complications, such as cerebral edema, are not as predictable but are very important.
Indeed, cerebral edema is the most important cause of mortality and long-term morbidity in patients with diabetic ketoacidosis. [12] The overall risk of cerebral edema is 1%, [1] with the condition occurring in 0.4% of established cases and in 1.2% of newly diagnosed cases. Mortality is high, approximately 20-25%, [1] with permanent neurologic deficits in 35% or more of survivors. [31, 9]
Other rare complications of diabetic ketoacidosis include acute respiratory distress syndrome (ARDS) with pulmonary edema, [34, 35] pneumomediastinum (secondary to hyperventilation), rhabdomyolysis, and acute renal failure. Patients with type 1 diabetes mellitus and diabetic ketoacidosis often suffer acute kidney injury, a more severe course occurring in those with a longer duration of type 1 diabetes and a higher anion gap measurement. [36] In addition, acute kidney injury and neurocognitive outcomes are not only associated with diabetic ketoacidosis in children, but they are more likely to affect those with greater acidosis and circulatory volume depletion. [37, 38]
Diabetic ketoacidosis during pregnancy is associated with a very high risk of fetal loss.
-
Pediatric Diabetic Ketoacidosis. Glasgow Coma Scale, modified for age of verbal response.
-
Pediatric Diabetic Ketoacidosis. A graphical representation of the electrocardiographic changes of hypokalemia.
-
Pediatric Diabetic Ketoacidosis. A graphical representation of the electrocardiographic changes of hyperkalemia (due to overcorrection of potassium loss).
-
Pediatric Diabetic Ketoacidosis. Diabetic ketoacidosis treatment and results chart (page 1 of 4).
-
Pediatric Diabetic Ketoacidosis. Diabetic ketoacidosis treatment and results chart (page 2 of 4).
-
Pediatric Diabetic Ketoacidosis. Diabetic ketoacidosis treatment and results chart (page 3 of 4).
-
Pediatric Diabetic Ketoacidosis. Diabetic ketoacidosis treatment and results chart (page 4 of 4).
-
Pediatric Diabetic Ketoacidosis. Carbs for Kids-Count Them In: The Constant Carbohydrates Diet.
-
Pediatric Diabetic Ketoacidosis. Diabetes Sick Day Rules.
-
Pediatric Diabetic Ketoacidosis. Taking Diabetes Back to School.
Tables
|
Mild (< 3%) |
Moderate (3-8%) |
Severe (8%) and Shock (>10%) |
Appearance |
Thirsty, alert |
Thirsty, lethargic |
Drowsy, cold |
Tissue turgor |
Normal |
Absent |
Absent |
Mucous membranes |
Moist |
Dry |
Very dry |
Blood pressure |
Normal |
Normal or low |
Low for age |
Pulse |
Normal |
Rapid |
Rapid and weak |
Eyes |
Normal |
Sunken |
Grossly sunken |
Anterior fontanelle |
Normal |
Sunken |
Grossly sunken |
Weight |
Infusion rate |
0-12.9 kg |
80 mL/kg/24 h |
13-19.9 kg |
65 mL/kg/24 h |
20-34.9 kg |
55 mL/kg/24 h |
35-59.9 kg |
45 mL/kg/24 h |
Adult (>60 kg) |
35 mL/kg/24 h |
Serum/Plasma K+ (mEq/L) |
Potassium Chloride (KCL) Dose in Infusion Fluids |
< 2.5 mEq/L |
Carefully monitored administration of 1 mEq/kg body weight by separate infusion over 1 h |
2.5-3.5 mEq/L |
40 mEq/L |
3.5-5 mEq/L |
20 mEq/L |
5-6 mEq/L |
10 mEq/L (optional) |
Over 6 mEq/L |
Stop K+ and repeat level in 2 h |



