Background
Several types of vascular rings have aortic arches that are right sided. Although the specific anatomic details of the various forms differ, they share the defining feature of all vascular rings, namely, encirclement of the trachea and esophagus by connected segments of the aortic arch and its branches. A right aortic arch may occur without forming a vascular ring. [1] The presence or absence of a vascular ring in the setting of a right aortic arch depends on the branching of the brachiocephalic vessels and the location of the ductus arteriosus, as discussed below.
It is important for clinicians to diagnose and properly define the anatomy of a vascular ring.
Embryology
The easiest way to understand the anatomy and development of vascular rings with a right aortic arch is to begin by considering the bilateral system of pharyngeal arch vessels in the early embryo.
Early in the course of embryonic morphogenesis, six pairs of pharyngeal arch arteries develop in conjunction with the branchial pouches. The first through sixth arches appear in more or less sequential fashion, with left-right symmetry, and constitute the primitive vascular supply to the brachiocephalic structures, running from the aortic sac to the paired dorsal aortas. As normal cardiovascular morphogenesis proceeds, a patterned regression and persistence of the various arches and right-sided dorsal aorta occur, ultimately resulting in the mature configuration of the thoracic aorta and its branches. The third, fourth, and sixth arches, along with the seventh intersegmental arteries and the left dorsal aorta, are the primary contributors to the normal aortic arch and its major thoracic branches (see image below).
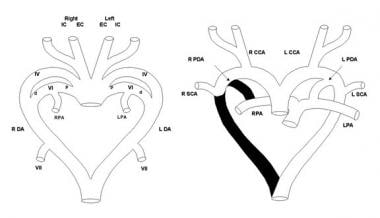 Left: Schematic diagram of the primitive pharyngeal arch system showing the left (L) and right (R) external carotid (EC) and internal carotid (IC) arteries, the fourth (IV) and sixth (VI) pharyngeal arches, distal pulmonary arterial segments (PA), dorsal aortas (DA), and seventh intersegmental arteries (VII). The proximal (p) sixth arches develop into the proximal pulmonary arteries, and the distal (d) sixth arches become the arterial ducts. The seventh intersegmental arteries develop into the subclavian arteries. Right: Schematic diagram depicting the segments of the pharyngeal arch system that regress (shown in black) in order for normal development of the great arteries and their thoracic branches (common carotid artery [CCA], left pulmonary artery [LPA], ductus arteriosus [PDA], right pulmonary artery [RPA], subclavian artery [SCA]).
Left: Schematic diagram of the primitive pharyngeal arch system showing the left (L) and right (R) external carotid (EC) and internal carotid (IC) arteries, the fourth (IV) and sixth (VI) pharyngeal arches, distal pulmonary arterial segments (PA), dorsal aortas (DA), and seventh intersegmental arteries (VII). The proximal (p) sixth arches develop into the proximal pulmonary arteries, and the distal (d) sixth arches become the arterial ducts. The seventh intersegmental arteries develop into the subclavian arteries. Right: Schematic diagram depicting the segments of the pharyngeal arch system that regress (shown in black) in order for normal development of the great arteries and their thoracic branches (common carotid artery [CCA], left pulmonary artery [LPA], ductus arteriosus [PDA], right pulmonary artery [RPA], subclavian artery [SCA]).
The segments of the bilateral aortic arch system that normally regress include the distal portion of the sixth arch and the right-sided dorsal aorta. Normally, the left fourth arch becomes the aortic arch, the right fourth arch contributes to the innominate artery, the distal left sixth arch becomes the ductus arteriosus, the proximal sixth arches bilaterally contribute to the proximal branch pulmonary arteries, the left dorsal aorta becomes the descending thoracic aorta, and the dorsal intersegmental arteries bilaterally become the subclavian arteries.
Vascular rings are formed when this process of regression and persistence does not occur normally, and the resulting vascular anatomy completely encircles the trachea and esophagus. (Other forms of aortic arch anomaly occur in which a vascular ring is not present.) A right aortic arch is formed when the right dorsal aorta remains patent and either the left fourth arch or the left dorsal aorta regress abnormally (see image below).
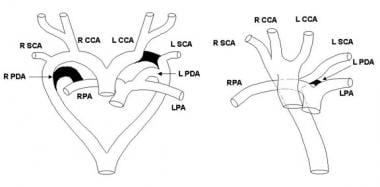 Left: Schematic diagram depicting the segments of the pharyngeal arch system that regress (shown in black) in order for the development of a right aortic arch with aberrant left subclavian artery. Abbreviations are as in the first image. Right: Mature anatomy of a vascular ring formed by a right aortic arch with an aberrant left subclavian artery arising from a retroesophageal diverticulum with a left-sided ligamentum arteriosum to the left pulmonary artery.
Left: Schematic diagram depicting the segments of the pharyngeal arch system that regress (shown in black) in order for the development of a right aortic arch with aberrant left subclavian artery. Abbreviations are as in the first image. Right: Mature anatomy of a vascular ring formed by a right aortic arch with an aberrant left subclavian artery arising from a retroesophageal diverticulum with a left-sided ligamentum arteriosum to the left pulmonary artery.
Anatomy
Vascular ring with a right aortic arch has two primary forms and two other forms that are much less common.
In the most frequent form of vascular ring with a right aortic arch, an aberrant origin of the left subclavian artery from a retroesophageal diverticulum (diverticulum of Kommerell) is present, which originates as the last branch of the aortic arch (distal to the right subclavian artery). [2] The ring is completed by a left-sided ductus arteriosus (or its remnant ligamentum arteriosum) passing from the aberrant left subclavian artery to the proximal left pulmonary artery (see image below).
Left: Schematic diagram depicting the segments of the pharyngeal arch system that regress (shown in black) in order for the development of a right aortic arch with aberrant left subclavian artery. Abbreviations are as in the first image. Right: Mature anatomy of a vascular ring formed by a right aortic arch with an aberrant left subclavian artery arising from a retroesophageal diverticulum with a left-sided ligamentum arteriosum to the left pulmonary artery.
The retroesophageal diverticulum is distinguished from the aberrant left subclavian artery by its larger caliber. Although the course of the descending thoracic aorta varies, it typically crosses gradually to the left of the vertebral column to pass through the diaphragm in the usual location of the aortic hiatus.
In the second major type of vascular ring with a right aortic arch, the brachiocephalic vessels originate from the arch in mirror-image fashion with the left innominate artery the first branch followed by the right common carotid and subclavian arteries. A left-sided ductus arteriosus or ligamentum arteriosum passes between the descending aorta and the proximal left pulmonary artery.
In contrast to right aortic arch with aberrant left subclavian artery from a retroesophageal diverticulum, the descending aorta usually crosses to the left side of midline proximally in its course, although in rare cases, it remains to the right of midline until reaching the lower portion of the thorax.
A rare form of vascular ring with a right aortic arch is a right arch with an aberrant retroesophageal innominate artery arising as the last branch of the arch and then giving off a ductus/ligamentum to the proximal left pulmonary artery (see image below).
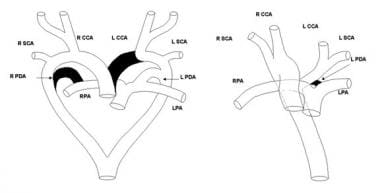 Left: Schematic diagram depicting the segments of the pharyngeal arch system that regress (shown in black) in order for the development of a right aortic arch with aberrant retroesophageal left innominate artery. Abbreviations are as in the first image. Right: Mature anatomy of a vascular ring formed by a right aortic arch with an aberrant retroesophageal left innominate artery with a left-sided ligamentum arteriosum to the left pulmonary artery.
Left: Schematic diagram depicting the segments of the pharyngeal arch system that regress (shown in black) in order for the development of a right aortic arch with aberrant retroesophageal left innominate artery. Abbreviations are as in the first image. Right: Mature anatomy of a vascular ring formed by a right aortic arch with an aberrant retroesophageal left innominate artery with a left-sided ligamentum arteriosum to the left pulmonary artery.
With this form of vascular ring, the retroesophageal innominate artery does not arise from a diverticulum.
An uncommon form of right aortic arch that technically is not a vascular ring but may cause symptoms similar to a ring is a right arch with an aberrant left subclavian artery arising as the last branch of the arch and a left-sided descending aorta. The ductus arteriosus is right sided; thus, a ring is not actually formed, but the retroesophageal descending aorta may rarely cause symptomatic airway symptoms, esophageal symptoms, or both.
Associated cardiovascular anomalies
Vascular rings, including those with a right aortic arch, usually occur without associated cardiovascular anomalies. Ventricular septal defect is the most common associated anomaly, although various others have been reported as well.
Associated syndromes and noncardiac conditions
Vascular ring with a right aortic arch is associated with a band 22q11 deletion in approximately 20% of patients (see Etiology). Band 22q11 deletion is responsible for DiGeorge, velocardiofacial, and conotruncal anomaly face syndromes, which are often referred to by the unified terms CATCH-22 syndrome or chromosome 22q11 deletion syndrome. In patients with vascular rings, the frequency of phenotypes satisfying the clinical criteria for these various syndromes is not known. The important point, rather, is that vascular rings with a right aortic arch may be associated with band 22q11 deletion, which has various other possible manifestations. These include, but are not limited to, palatal abnormalities, laryngotracheal anomalies, speech and learning delay, characteristic facial features, hypocalcemia, abnormalities of T-cell–mediated immune function, and neurologic defects.
Occasionally, patients with right aortic arch may have anomalies consistent with either vertebral, anal, cardiac, tracheal, esophageal, renal, and limb (VACTERL) associations or posterior coloboma, heart defect, choanal atresia, retardation, genital, and ear (CHARGE) associations. One of the more important noncardiac features that is sometimes found in association with right aortic arch is esophageal atresia, insofar as an undiagnosed arch anomaly may complicate repair of the esophageal atresia, which is usually recognized earlier than the right aortic arch.
Congenital laryngeal web is another noncardiac anomaly that may be associated with vascular rings and may present with the same symptoms and signs as a vascular ring. Accordingly, patients with persistent stridor, upper airway obstruction, or both after repair of a vascular ring, particularly those with a chromosome 22q11 deletion, should be evaluated for the presence of a congenital laryngeal web.
Epidemiology
United States data
The incidence of right aortic arch and vascular rings in general is not known, although vascular rings comprise an estimated 1% of cardiovascular malformations managed surgically.
Race-, sex-, and age-related demographics
Based on limited data, no racial predilection is apparent.
No sex predilection of vascular rings with right aortic arch has been documented.
A right aortic arch is a developmental abnormality that is present in the fetus. The postnatal age at which this anomaly is identified may vary, although most patients are identified in early infancy. A right aortic arch with vascular ring can also be identified on prenatal echocardiography. [3]
Etiology
Factors responsible for aberrant development of the aortic arch and its branches, as occurs in patients with vascular rings, have not been clearly identified, and the pathogenesis of these anomalies remains unclear. Vascular rings with a right aortic arch typically occur without associated cardiovascular defects, although other lesions may be present, and accordingly are not usually found as part of a syndromic complex. No methods are known that prevent the development of vascular ring with a right aortic arch.
Chromosomal anomaly
In a study from the author's institution, band 22q11 deletions were found in 8 of 34 patients (24%) with a right aortic arch, vascular ring, and no other cardiac defects. [4] The deletion was found in 8 of 29 patients (28%) with a right arch, aberrant left subclavian artery, and left-sided ductus from the aberrant left subclavian artery to the left pulmonary artery and in none of 5 patients with a right arch, mirror-image branching of the brachiocephalic vessels, and a left ductus from the descending aorta to the left pulmonary artery.
This chromosomal anomaly is associated with aortic arch anomalies in patients with other forms of conotruncal heart disease as well as other isolated vascular abnormalities, and band 22q11 deletion is likely an important etiologic factor in vascular rings with a right aortic arch.
Although band 22q11 deletion was not found in 5 patients with a vascular ring formed by a mirror-image right arch and a left ductus from the descending aorta, this sample is too small to rule out a potential association.
In general, most band 22q11 deletions arise de novo, and no recognizable inheritance pattern is present.
Aortic arch anomalies
Aortic arch anomalies, including vascular rings, have been induced in various animal models, such as neural crest–ablated chicks, mice with disrupted genes for the endothelin-A receptor or endothelin-converting enzyme, and others. The mechanisms and significance of these models for understanding the development of vascular rings have not been elucidated.
Pathophysiology
Vascular rings, by definition, encircle the trachea and esophagus, usually causing compression of both structures. [5] Compression of the trachea causes upper airway obstruction that impairs inspiratory and, to a lesser degree, expiratory airflow. The extent of respiratory impairment depends on the severity of compression, which can widely vary. Symptomatic compression of the trachea seems to occur slightly later in life with vascular rings having a right aortic arch when compared to vascular rings with double aortic arch.
In addition to airway symptoms, patients may experience swallowing problems related to esophageal compression. These typically manifest as vomiting and feeding intolerance in infants and younger children and as dysphagia later in life. Swallowing dysfunction may contribute to respiratory symptoms as a result of aspiration and/or compression or irritation of the membranous portion of the trachea as a food bolus traverses the area of esophageal obstruction. Although respiratory or esophageal pathophysiology may predominate in any given patient, respiratory compromise is generally more problematic in younger patients. Those with primarily esophageal symptomatology tend to be older at presentation. The pathophysiology of vascular rings with a right aortic arch does not differ among the various anatomic forms.
Prognosis
The long-term prognosis for patients with repaired vascular rings is excellent, with persistent respiratory symptoms being the most common adverse outcome.
Morbidity/mortality
The natural history of vascular rings in general, including those with a right aortic arch, is not well defined. Vascular rings were among the first congenital cardiovascular anomalies repaired surgically, and surgical management has been the standard of care for more than 50 years. Patients with significant airway compression may die as a result of respiratory compromise, but such events are rare.
Preoperative morbidity is generally limited to respiratory symptoms, feeding problems, or both. Some patients may develop recurrent respiratory infections, and some may exhibit failure to thrive because of the combination of increased metabolic requirements from respiratory and feeding work and relatively poor oral intake.
Complications
Complications are uncommon after repair of vascular rings.
The major postoperative issue is persistent respiratory symptoms, including cough, dyspnea, and wheezing. Pulmonary function testing reveals persistent upper airway obstruction in some patients. Others have evidence of lower airway obstruction that is generally responsive to bronchodilator therapy. Whether the incidence of lower airway obstruction is higher in patients who have undergone repair of vascular rings than in the general population or whether such pathology in patients with rings has any relationship to their prior anatomic and functional abnormalities is not known.
Rarely, patients with tight unrepaired rings may develop aortoesophageal fistula, which may lead to life-threatening hemorrhage. [6]
Patient Education
For the early posthospital period, parents must be educated about the possible persistence of symptoms, the potential benefit of prone positioning in patients with tracheomalacia, signs and symptoms of aspiration, and management of the thoracotomy incision.
No dietary or activity restrictions are indicated after repair of an isolated vascular ring.
In patients with a repaired vascular ring, lifestyle implications are minimal and are most likely related to residual symptoms or associated anomalies.
No special issues or concerns related to pregnancy in patients with repaired vascular ring exist. In patients with an unrepaired ring, pregnancy-induced physiologic changes should not be of special concern, although symptoms may be exacerbated in certain situations.
-
Left: Schematic diagram of the primitive pharyngeal arch system showing the left (L) and right (R) external carotid (EC) and internal carotid (IC) arteries, the fourth (IV) and sixth (VI) pharyngeal arches, distal pulmonary arterial segments (PA), dorsal aortas (DA), and seventh intersegmental arteries (VII). The proximal (p) sixth arches develop into the proximal pulmonary arteries, and the distal (d) sixth arches become the arterial ducts. The seventh intersegmental arteries develop into the subclavian arteries. Right: Schematic diagram depicting the segments of the pharyngeal arch system that regress (shown in black) in order for normal development of the great arteries and their thoracic branches (common carotid artery [CCA], left pulmonary artery [LPA], ductus arteriosus [PDA], right pulmonary artery [RPA], subclavian artery [SCA]).
-
Left: Schematic diagram depicting the segments of the pharyngeal arch system that regress (shown in black) in order for the development of a right aortic arch with aberrant left subclavian artery. Abbreviations are as in the first image. Right: Mature anatomy of a vascular ring formed by a right aortic arch with an aberrant left subclavian artery arising from a retroesophageal diverticulum with a left-sided ligamentum arteriosum to the left pulmonary artery.
-
Left: Schematic diagram depicting the segments of the pharyngeal arch system that regress (shown in black) in order for the development of a right aortic arch with mirror-image branching of the brachiocephalic vessels and a left-sided ductus arteriosus from the descending aorta to the left pulmonary artery. Abbreviations are as in the first image. Right: Mature anatomy of a vascular ring formed by a right aortic arch with mirror-image branching of the brachiocephalic vessels and a left-sided ductus arteriosus from the descending aorta to the left pulmonary artery.
-
Left: Schematic diagram depicting the segments of the pharyngeal arch system that regress (shown in black) in order for the development of a right aortic arch with aberrant retroesophageal left innominate artery. Abbreviations are as in the first image. Right: Mature anatomy of a vascular ring formed by a right aortic arch with an aberrant retroesophageal left innominate artery with a left-sided ligamentum arteriosum to the left pulmonary artery.





