Background
Zollinger-Ellison syndrome (ZES) is a rare condition characterized by peptic ulcers that are refractory to conventional medical therapy. Gastrin-producing tumors or gastrinomas cause excessive gastric acid secretion, leading to these ulcers of the upper gastrointestinal (GI) tract, as well as diarrhea and severe abdominal pain (see the following image). [1]
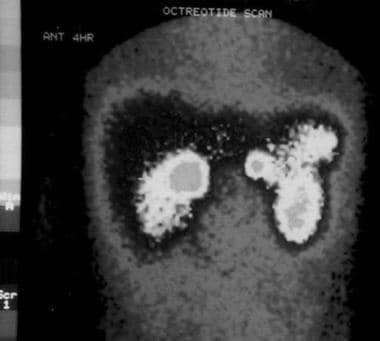 Somatostatin receptor scintigraphy in a young patient with Zollinger-Ellison syndrome. Besides physiologic uptake in the kidneys and the spleen, 2 pathologic hot spots are present, one in the area of the duodenum and another next to the pancreas.
Somatostatin receptor scintigraphy in a young patient with Zollinger-Ellison syndrome. Besides physiologic uptake in the kidneys and the spleen, 2 pathologic hot spots are present, one in the area of the duodenum and another next to the pancreas.
Childhood gastrinomas account for about 2% of all Zollinger-Ellison syndrome cases in the United States. The overall incidence of gastrinomas occurring sporadically or in association with multiple endocrine neoplasia type 1 (MEN-1) is 0.1-3 per million; the prevalence of MEN-1 is 0.2-2 cases per 100,000 population. MEN-1 is diagnosed in 30-38% of patients with gastrinomas, whereas 20-61% of patients diagnosed with MEN-1 are found to have gastrinomas associated with Zollinger-Ellison syndrome.
Until 1992, 60 cases of Zollinger-Ellison syndrome in children had been reported worldwide.
In 2004, Gibril et al published a large, prospective study of 107 patients with Zollinger-Ellison syndrome associated with MEN-1 and reported that 78% of patients were white, 10% were black, and 9% were Hispanic. [2] The incidence of this disease in male children is 4 times greater than that of female children, which is in contrast to Zollinger-Ellison syndrome in adults, in which a slight male predominance is noted. [3]
The youngest patient reported with Zollinger-Ellison syndrome was a boy aged 7 years. Gastrinomas have been found in patients aged 90 years and younger, with the most common age at diagnosis being 30-50 years.
This syndrome was originally described by Zollinger and Ellison in 1955. [4] In 1960, Cawkwell described the first childhood case of Zollinger-Ellison syndrome in The New Zealand Medical Journal.
See also Pediatric Multiple Endocrine Neoplasia, Pediatric VIPoma, Gastrinoma, Zollinger-Ellison Syndrome, Wermer Syndrome (MEN Type 1), and Peptic Ulcer Disease.
Etiology and Pathophysiology
Gastrinomas may be sporadic or may be associated with multiple endocrine neoplasia type 1 (MEN-1). Data suggest that the gene for MEN-1, called MENIN, is also involved in the pathogenesis of at least one third of sporadic neuroendocrine tumors (NETs), including gastrinomas. Therefore, all patients who are under evaluation for Zollinger-Ellison syndrome (ZES) should undergo genetic testing for MEN-1.
MEN-1 is known to cause multiple tumors within the pancreas, pituitary, parathyroid, and adrenal glands through an autosomal dominant pattern of inheritance. Patients with MEN-1 may also have an increased risk of skin lesions and carcinoid and smooth muscle tumors. MEN-1 is due to mutations in the tumor suppressor gene MEN1, located on chromosome 11q13. MEN1 encodes a transcriptional regulator protein, menin. Patients with MEN-1 have one germline mutation and one somatic mutation that lead to inactivation of menin.
Gastrinomas are neuroendocrine tumors that are usually found in the duodenum wall (approximately 50%) or in the pancreas. Approximately 85% of gastrinomas are located in the gastrinoma triangle, which is superiorly bound by the confluence of the cystic and common bile duct, inferiorly bound by the second and third portions of the duodenum, and medially bound by the head and body of the pancreas. [5] When gastrinomas are found in the pancreas, they are non–beta islet cell tumors. However, in addition to locations in the duodenum and pancreas, gastrinomas have been described in the lymph nodes, liver/biliary tree, gastric antrum, and jejunum. Rare reports have described extra-gastrointestinal (GI) gastrinomas occurring in the heart, ovaries, lung, splenic hilum, and renal capsule. [6]
Gastrinomas are the second most common neuroendocrine tumors in the overall population, after insulinomas and before vasoactive intestinal polypeptide tumors (VIPomas) and glucagonomas. Gastrinomas may secrete not only high levels of gastrin, causing peptic ulcer disease (PUD) but also may secrete other hormones such as adrenocorticotropic hormone (ACTH), vasoactive intestinal polypeptide (VIP), and glucagon. Gastrinomas may also produce various peptides such as insulin, pancreatic polypeptide, glucagon, chromogranin A, neuron-specific enolase, and the alpha and beta subunits of human chorionic gonadotropin (HCG).
Carcinoid tumors are GI neuroendocrine tumors that are mostly indolent; however, they may secrete various hormones and biogenic amines that cause carcinoid syndrome. [7] Gastric carcinoids (type 2 carcinoids) occur almost exclusively in patients with MEN-1 who have Zollinger-Ellison syndrome (21–30% of patients with MEN-1) and can be malignant in 10–30% of cases. [8]
Prognosis
Before the introduction of acid-suppressing drugs, including histamine H2-receptor antagonists and, more recently, proton pump inhibitors (PPIs), Zollinger-Ellison syndrome (ZES) carried high mortality rates. Because safe control of gastric acid hypersecretion can be achieved with PPIs in virtually all patients, mortality and morbidity are now attributed to advanced disease with metastases to liver and bones. [9] Due to small numbers, it is not clear whether gastrinoma tumor growth in children is less aggressive than in adults, as previously thought.
In a study from the National Institutes of Health (NIH) involving 151 patients with Zollinger-Ellison syndrome, the 10-year survival rate was 94% in the overall Zollinger-Ellison syndrome population. [10] The survival rate at 10 years was slightly lower (89%) when Zollinger-Ellison syndrome was associated with multiple endocrine neoplasia type 1 (MEN-1). In the latter condition, a high prevalence of gastric carcinoids has been described; these carcinoids can be malignant in 10–30% of cases; thus, they require active surveillance to prevent increased mortality.
Gastrinomas may be malignant or benign, but they are typically slow growing. Early studies reported malignancy rates as high as 65% in adults. More recent studies report a malignancy rate of closer to 30%. Lymph nodes, liver, and bone metastases are the most common, although occurrence rates in children are unknown. One case report described a renal gastrinoma in a 12-year-old child. [11]
Approximately 60% of gastrinomas are benign at the time of diagnosis, without metastases. Because of the small size of gastrinomas, cure (disease free for at least 5 y) is achieved in only 20-40% of cases.
The development of liver metastases, especially a rapidly enlarging metastatic lesion, is considered an unfavorable sign; however, depending on the tumor biology, patients with liver metastases have survived 10 years and longer. Patients with gastrinomas releasing adrenocorticotropic hormone (ACTH), which causes Cushing syndrome, or who have bone metastasis also have a poor prognosis and should receive antitumor treatment. [3]
Complications
With the introduction of PPIs that are effective in almost all patients, acid-related complications are now reduced to a minimum. Complications of peptic ulcer disease (PUD) before the diagnosis include perforation, bleeding, and esophagitis. A stricture of the gastroesophageal junction may develop.
-
Somatostatin receptor scintigraphy in a young patient with Zollinger-Ellison syndrome. Besides physiologic uptake in the kidneys and the spleen, 2 pathologic hot spots are present, one in the area of the duodenum and another next to the pancreas.
-
Somatostatin receptor scintigraphy in a young patient with Zollinger-Ellison syndrome whose gastrinomas were resected. The LEFT (big) tumor was a periduodenal lymph node gastrinoma; the RIGHT tumor was a pancreatic gastrinoma. Despite negative findings on the scan, the patient remained hypergastrinemic, probably because of microscopic disease that escaped diagnostic imaging and surgical exploration.







