Practice Essentials
Mycoplasmal organisms are the smallest known free-living life forms. They are nearly ubiquitous in both the plant and animal kingdoms as colonizers and pathogens. They are prokaryotes but lack a cell wall. [1] However, they have a unique cell membrane that contains sterols, which are not present in either bacteria or viruses. Mycoplasma organisms are small (150-250 nm) and have deformable membranes. The name Mycoplasma refers to the plasticity of the bacterial forms resembling fungal elements.
When they were first discovered, mycoplasmal organisms were believed to be viruses because they pass through filters that retain bacteria. However, unlike viruses, they are able to grow in cell-free media and contain both RNA and DNA. Mycoplasma species have also been mistakenly believed to be L-forms of bacteria, which also lack cell walls. Unlike mycoplasmal organisms, L-form bacteria do not have sterols in the cell membranes, and they can revert to their walled parental forms. The following summary is modified from Baum's "Introduction to Mycoplasma Diseases" in Principles and Practice of Infectious Diseases (see the image below). [2]
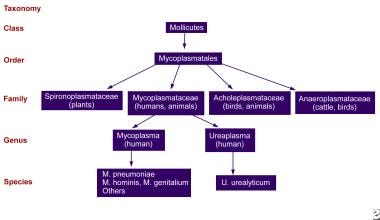 General characteristics of Mycoplasma species.
General characteristics of Mycoplasma species.
The general characteristics of Mycoplasma species include the following:
-
Prokaryotic
-
Size of 150-250 nm
-
Lack of a cell wall
-
Sterol-containing cell membrane
-
Fastidious growth requirements
-
Fried-egg or mulberry colonies on agar
Mycoplasma species differ from viruses in the following ways:
-
They grow on cell-free media in vitro.
-
They contain both RNA and DNA.
-
They have both intracellular and extracellular parasitism in vivo.
Mycoplasma species differ from bacteria (including L-forms) in the following ways:
-
They have sterols in the cell membrane.
-
They share no DNA homology with known bacteria.
-
They have low guanine levels plus cytosine content.
-
Their genome has a low molecular weight.
-
They exhibit no reversion to walled forms.
Mycoplasma pneumoniae causes infections leading to clinically apparent disease involving the upper respiratory tract. In 5-10% of patients, depending on age, the infection progresses to tracheobronchitis or pneumonia. Mycoplasma hominis causes genital mycoplasmal infections, which may result in diverse manifestations.
Patient education regarding the common occurrence, relatively mild nature, appropriate therapy, and usually complete recovery from Mycoplasma infection is important.
Pathophysiology
Mycoplasma organisms cause infection primarily as extracellular parasites, attaching to the surface of ciliated and nonciliated epithelial cells of the respiratory and genital tracts. A unique group of membrane proteins allow this adherence. [3] The attachment site, or receptor, is a complex carbohydrate structurally akin to antigen I of RBCs. The antibody response to this receptor results in production of the anti-I antibody or cold agglutinin, which acts as an autoantibody. Following attachment, mycoplasmal organisms may cause direct cytotoxic damage to epithelial cells because of hydrogen peroxide generation or cytolysis via an inflammatory response mediated by mononuclear cells or antigen-antibody reactions.
Mycoplasma pneumoniae is one of the few Mycoplasma species that causes human disease. [4] Most M pneumoniae –associated illnesses are confined to the respiratory tract; however, M pneumoniae respiratory infections are also associated with various extrapulmonary manifestations. [5, 6, 7, 8, 9, 10] The pathogenesis of extrapulmonary complications is unknown but is thought to be an immunomediated mechanism. [11] Systemic spread of the bacterium is rare. Genital mycoplasmal organisms are associated with numerous genitourinary tract and reproductive diseases but also can cause infections at other sites. [2]
Genital mycoplasmal organisms (eg, Mycoplasma hominis, Mycoplasma fermentans, Mycoplasma genitalium, Ureaplasma species) are sexually transmitted. Colonization rates for M hominis and Ureaplasma species are 20-50% and 40-50%, respectively. These organisms are associated with numerous genitourinary tract and reproductive diseases and have been implicated in preterm labor and bacteremia in very preterm newborn infants. [12, 13, 14, 15]
Mycoplasmal organisms commonly contaminate tissue cultures, in which they act as intracellular parasites and alter both cellular and viral molecular events. They are difficult to eliminate, and they raise questions regarding the validity of molecular biology results from tissue-culture experiments. [2]
Epidemiology
United States statistics
The disease is distributed worldwide without regard to season. [4] Atypical organisms such as M pneumoniae are implicated in as many as 40% of cases of community-acquired pneumonia. [16, 17] In the United States, at least 1 case of mycoplasmal pneumonia per 1000 persons is estimated to occur each year, or more than 2 million cases annually. The rates are rising in the central United States. [18] The incidence may be much higher because most mild-to-moderate cases are treated empirically.
International statistics
One study focused on the epidemiological and clinical features of an M pneumoniae outbreak in a kindergarten class in Beijing, China. [19] The report determined that the outbreak was caused by poor ventilation in a temporary classroom.
Race-, sex-, and age-related demographics
Race
Patients with sickle cell disease or related hemoglobinopathies are at increased risk for severe M pneumoniae infections and may develop large pleural effusions and marked respiratory distress. [20] Those who develop extremely high cold agglutinin titers may experience digital necrosis. [2] Because sickle cell disease and other related hemoglobinopathies are most common among Blacks, severe complications of mycoplasmal infections also occur most frequently in this group of patients.
Genital Mycoplasma species have been isolated more frequently from Black men and women than from White men and women. [21] Ureaplasma species are found 4 times more often than M. hominis.
Sex
No effect is observed according to sex of the patient on the frequency or severity of M pneumoniae infections. Colonization with Ureaplasma organisms and M hominis primarily occurs as a result of sexual contact. Both have been found more often in women than in men and more often in infant girls than in infant boys. [11]
Age
Children younger than 3 years primarily develop upper respiratory tract infection. [22] M pneumoniae infection is uncommon in the first year of life; however in neonates, it may cause severe respiratory disease and extrapulmonary illness. [2] M. pneumoniae infection is common in school-aged children and adolescents, with the highest rate of infection in individuals aged 5-9 years, in whom the tendency is to develop bronchitis and pneumonia. [2] An outbreak in 2009 in Japan in 2 schools was attributed to the close contact of students. [23]
Colonization of infants by genital Mycoplasma species usually occurs during passage through an infected birth canal, and genital mycoplasmal organisms have been isolated from the upper respiratory tract in 15% of infants. [2] Colonization usually does not persist beyond 2 years. [11]
A population-based cross-sectional study that included 37 preschool and 55 school-age children who tested positive for M pneumoniae reported that compared to school-age children, preschool children infected with M. pneumoniae had significantly higher risk (60% vs 42%) of severe disease (severe pneumonia). [24]
Prognosis
Prognosis for Mycoplasma infections is usually excellent; however, if complications occur, long-term sequelae may result.
Morbidity/mortality
Most M pneumoniae infections lead to clinically apparent disease involving the upper respiratory tract; the symptoms include pharyngitis, cough, headache, chills, and myalgias. [2] In 5-10% of patients (with the rate depending on age), the infection progresses to tracheobronchitis or pneumonia and is usually self-limited. Pleural effusion (usually small) occurs in 5-20% of patients. [2] M pneumoniae has been strongly implicated in the pathogenesis of asthma, leading to acute and chronic wheezing in some individuals. [25, 26, 27, 28, 29]
Precedent M pneumoniae respiratory infections have also been implicated in patients who present with extrapulmonary illness. The most common sites of extrapulmonary manifestations are dermatologic (25%) and CNS (1-10%), although cardiac, musculoskeletal, hematologic, and GI symptoms have also been reported. [7, 9, 10]
Children with compromised immunity, including those with humoral immunodeficiencies, are more likely to experience complications. [4, 11] In individuals with sickle cell anemia, mycoplasmal infection may be severe, with acute chest syndrome reported. [20] Unusually severe M pneumoniae infection has also been reported in children with Down syndrome, especially those with congenital heart disease. [2]
Complications
Complications are relatively rare. See Physical Examination for further detail on extrapulmonary manifestations of M pneumoniae infection.
-
General characteristics of Mycoplasma species.









