Practice Essentials
A mallet toe is a fixed or flexible deformity of the distal interphalangeal (DIP) joint of the toe. [1] It is characterized by neutral positioning of the metatarsophalangeal (MTP) and proximal interphalangeal (PIP) joints in the face of a flexed DIP joint, [2] in contrast to the extended or neutral position of the MTP joint and flexed position of the PIP joint characterized by the more common hammertoe deformity. In certain patients with hammertoe deformity, the DIP can present in flexion. Given this overlap in presentation at the DIP joint, clinicians should be familiar with both conditions and be able to distinguish between them. [3]
Mallet toe is primarily a condition affecting the lesser toes; mallet toe of the hallux can occur but is quite rare. [4, 5]
Both pain and callosity may be the presenting complaints when the DIP joint of the toe has abnormal flexion, regardless of whether it is fixed or flexible.
Treatment of mallet toe deformity is relatively straightforward (see Treatment). Some controversy exists over the need for flexor tenotomy when DIP joint arthrodesis is attempted and the question of whether this leads to a higher incidence of hyperextension deformity and PIP joint flexion at the adjacent PIP joint.
For information on related topics, see Claw Toe and Hammertoe Deformity.
Anatomy
The DIP joint is a hinge joint with collateral and accessory collateral ligaments and a plantar plate. The flexor sheath extends to the DIP joint. [6, 7]
Pathophysiology
The principal pathophysiology is flexion of the DIP joint with pressure on the tip of the toe, often with associated attenuation of the extensor tendon (see the images below). This may lead to callosity or nail deformity on the tip of the toe. The deformity may be flexible in cases where the principal problem is an overtight flexor digitorum longus (FDL). However, the deformity is typically fixed in cases where the plantar joint structures are contracted or alteration of the joint surfaces restricting joint range of motion (ROM) has occurred. [8, 9, 10, 11]

 Radiograph of the same patient with an implant in the PIP joint causing a mallet deformity in the DIP joint.
Radiograph of the same patient with an implant in the PIP joint causing a mallet deformity in the DIP joint.
Etiology
Mallet toe deformity of a long toe is usually idiopathic. Inappropriate shoe wear, iatrogenic causes (eg, previous PIP joint fusion [12] ), congenital abnormalities, trauma, neuromuscular disorders, and pes cavus can all lead to the deformity. [13]
Epidemiology
In the United States, mallet toe deformity is much less common than hammertoe deformity, with a 1:9 ratio. It occurs most often in the second toe (75%) but can also occur in the remaining lesser toes. In as many as 12% of cases, associated lateral or medial deviation may be present.
The international incidence of mallet toe is unknown; however, population‐based studies in Australia and Sweden reported that surgical management of these deformities accounted for between 28% and 46% of all forefoot surgery performed in those countries. [14, 15]
Prognosis
In most series, 85-97% of cases have had excellent results after treatment. [16] In some series, tenotomy seemed to increase satisfaction rates. Bony union of the DIP joint had higher satisfaction rates than fibrous union did when resection was carried out.
-
Classic mallet toe. Note flexion when toe is dorsiflexed.
-
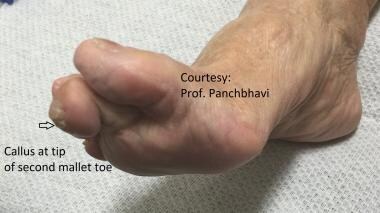
Photo showing acute flexion deformity at the DIP joint of the second toe.
-
Radiograph of the same patient with an implant in the PIP joint causing a mallet deformity in the DIP joint.



